CSF and meninges/ CSF and meninges/ CSF and meninges.pdf
1.
After 21 centuriesof scientific inquiry,
our understanding of cellular biology
has made significant progress, but the
percentage of nervous system cells for
which we fully understand all
functions is indeed relatively low
[almost 10%]. The 90%, are still under
exploration.
This study reportsa rare case of acute
obstructive hydrocephalus following
aqueductal stenosis.
An 11-year-old boy admitted to the
hospital with progressive headache,
nausea and vomiting throughout
a month.
5.
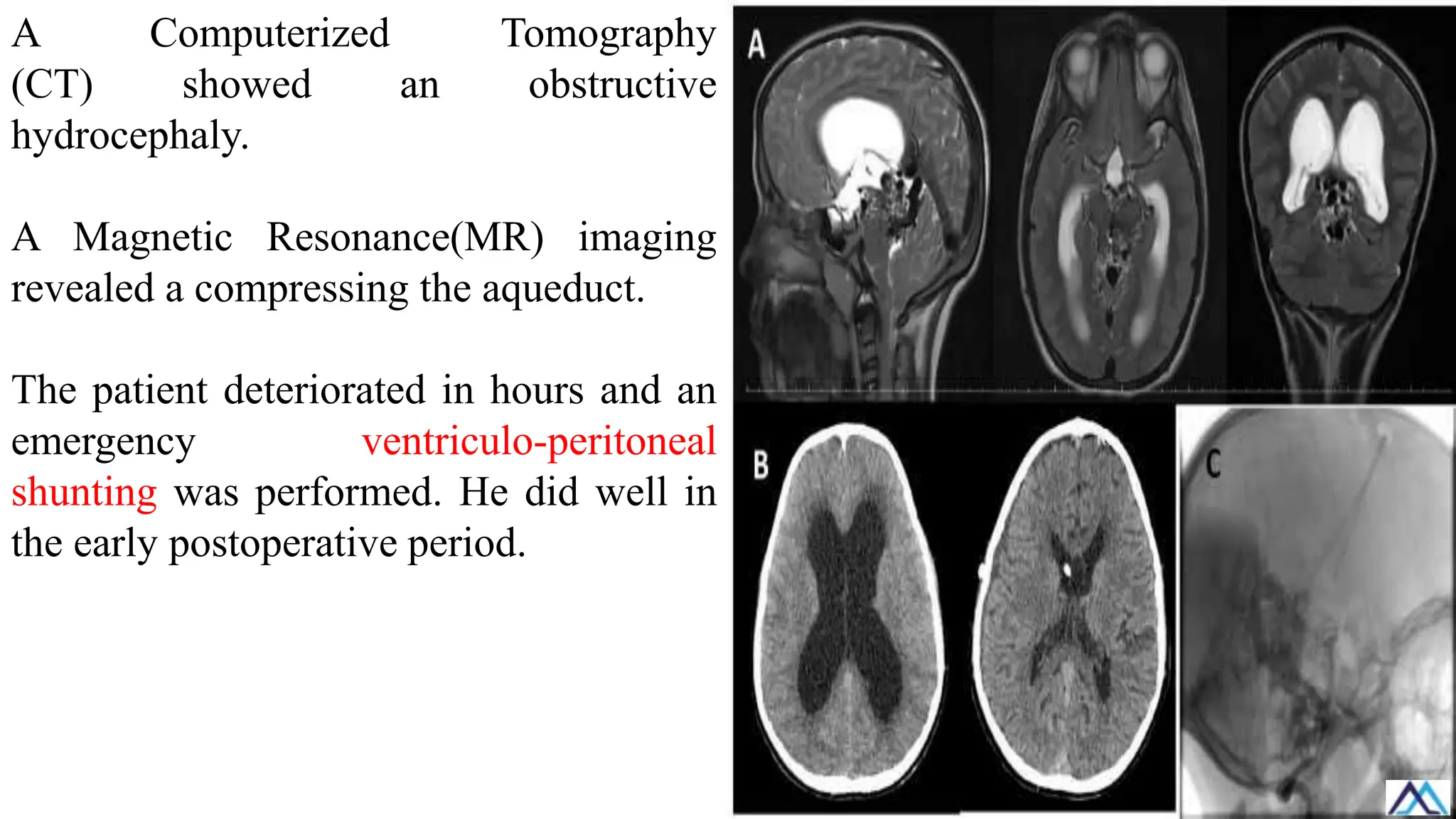
A Computerized Tomography
(CT)showed an obstructive
hydrocephaly.
A Magnetic Resonance(MR) imaging
revealed a compressing the aqueduct.
The patient deteriorated in hours and an
emergency ventriculo-peritoneal
shunting was performed. He did well in
the early postoperative period.
ILOs
A. Describe theAnatomy and Function of the Meninges: Students will be able to describe the anatomy of the meninges,
including the three protective layers surrounding the brain and spinal cord: the dura mater, arachnoid mater, and pia
mater. They will understand the structure and function of each layer, including how they contribute to protecting the
CNS and maintaining its structural integrity.
B. Explain the Production and Circulation of Cerebrospinal Fluid (CSF): Students will be able to explain how cerebrospinal
fluid (CSF) is produced by the choroid plexuses in the ventricles of the brain. They will describe the pathway of CSF
circulation through the ventricular system, its flow through the subarachnoid space, and its reabsorption into the
venous system via the arachnoid granulations.
C. Describe the Role of CSF in Maintaining CNS Homeostasis: Students will be able to describe the role of CSF in
maintaining CNS homeostasis, including its functions in cushioning the brain and spinal cord, removing metabolic
waste products, and providing a stable chemical environment for neural tissue. They will understand how CSF helps to
protect the CNS from mechanical injury and regulate intracranial pressure.
D. Identify and Interpret Clinical Procedures Related to CSF and Meninges: Students will be able to identify and interpret
clinical procedures related to CSF and the meninges, such as lumbar puncture (spinal tap) and imaging techniques
like CT and MRI. They will understand how these procedures are used to assess CSF composition, measure
intracranial pressure, and detect conditions affecting the meninges, such as meningitis or tumors.
9.
While the meningesthemselves are not
typically the direct target of surgical
procedures, they play a crucial role in
neurosurgery and other related
interventions. The meninges are the
protective layers surrounding the brain
and spinal cord, consisting of the dura
mater, arachnoid mater, and pia mater.
The surgical importance of the meninges
lies in their role as protective barriers and
their involvement in certain medical
conditions and procedure.
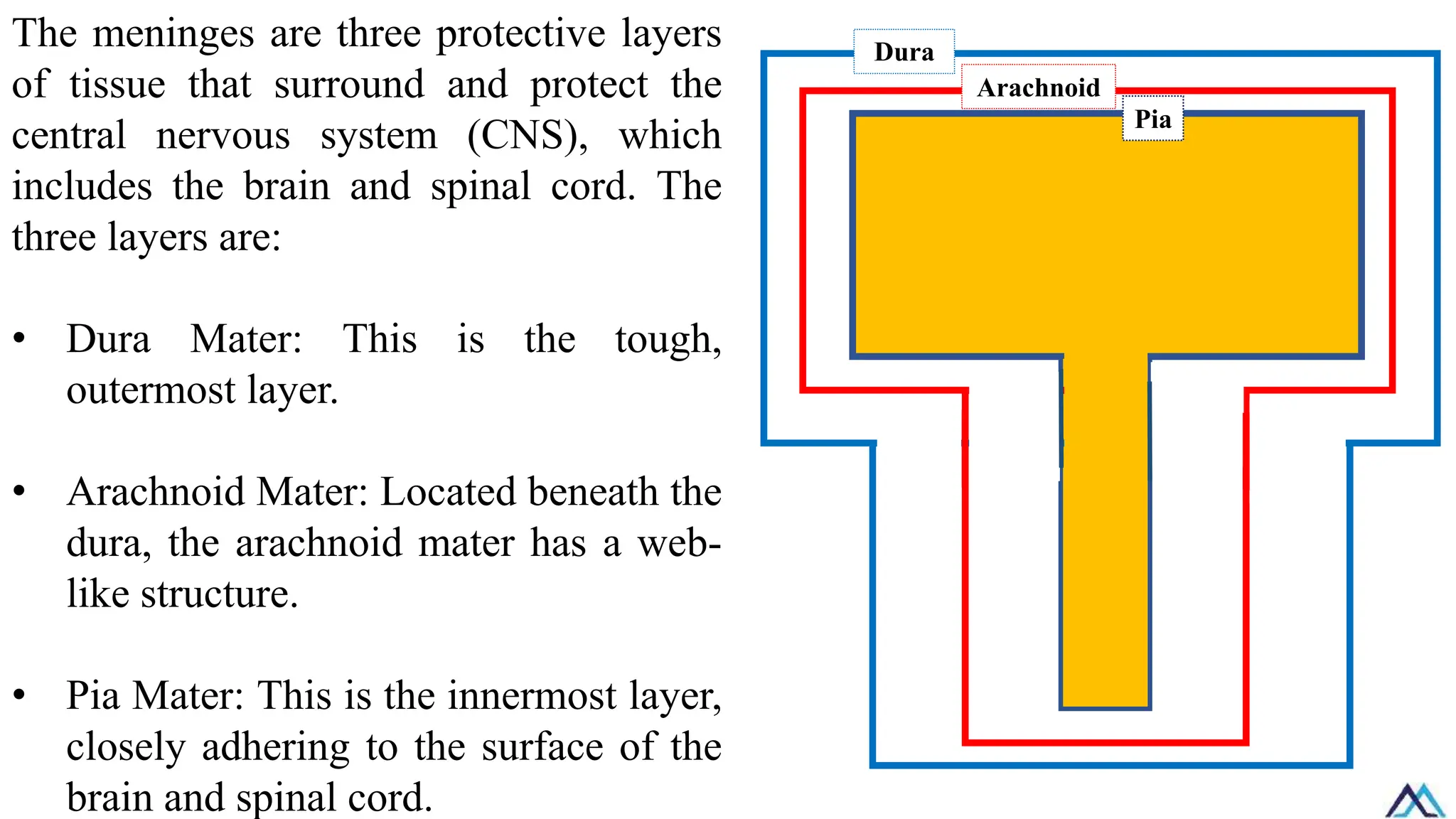
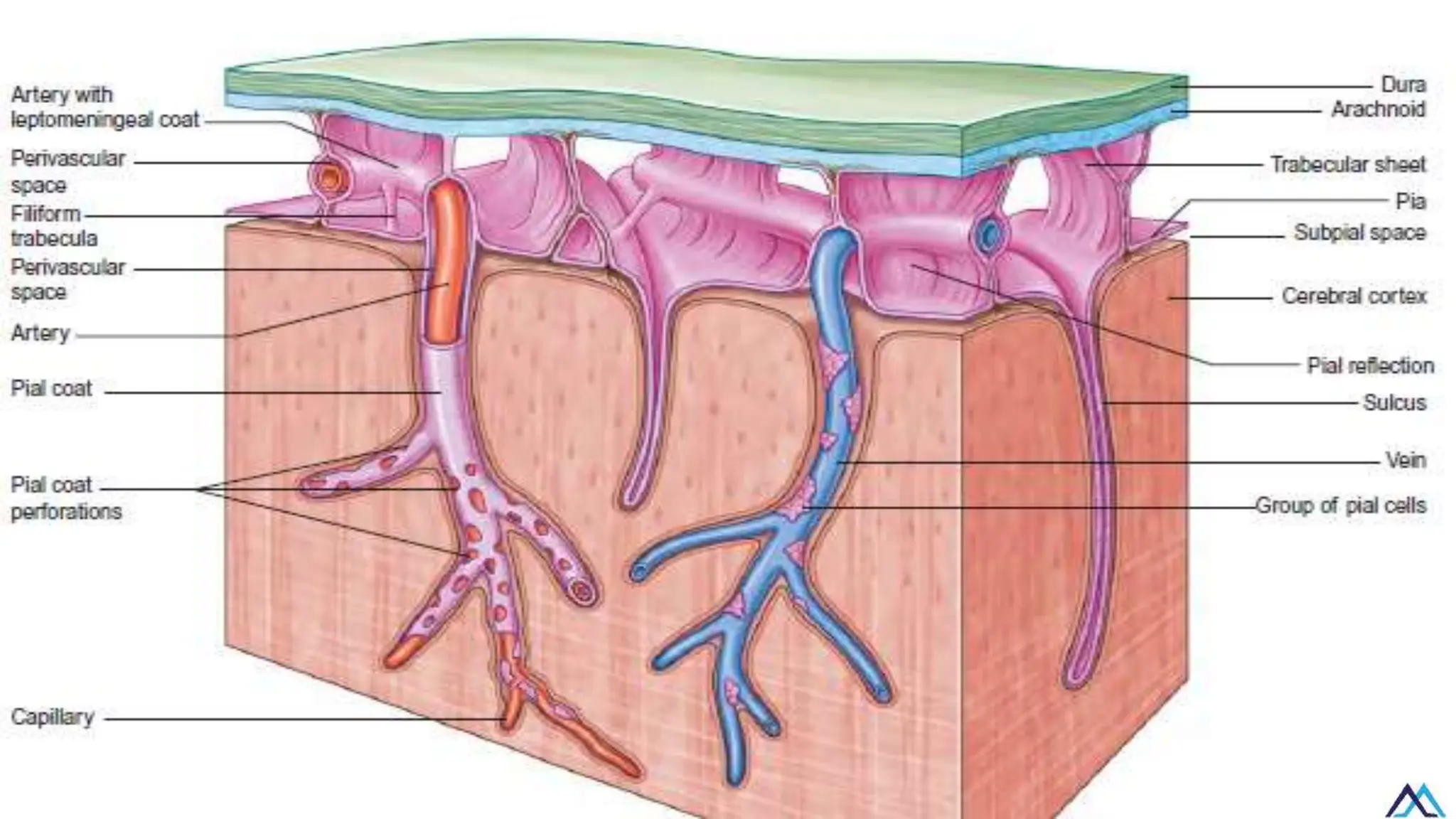
The meninges arethree protective layers
of tissue that surround and protect the
central nervous system (CNS), which
includes the brain and spinal cord. The
three layers are:
• Dura Mater: This is the tough,
outermost layer.
• Arachnoid Mater: Located beneath the
dura, the arachnoid mater has a web-
like structure.
• Pia Mater: This is the innermost layer,
closely adhering to the surface of the
brain and spinal cord.
Dura
Arachnoid
Pia
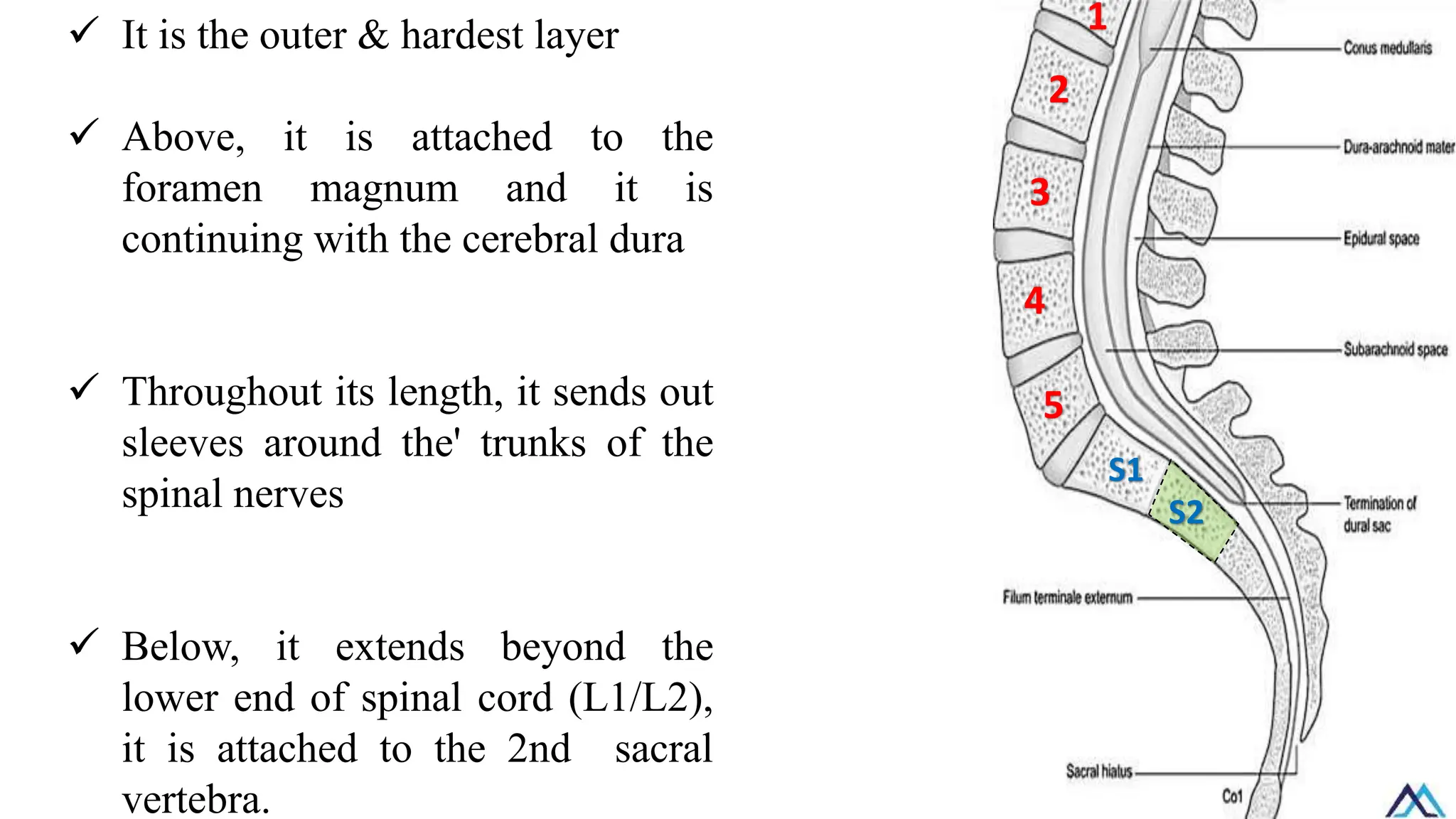
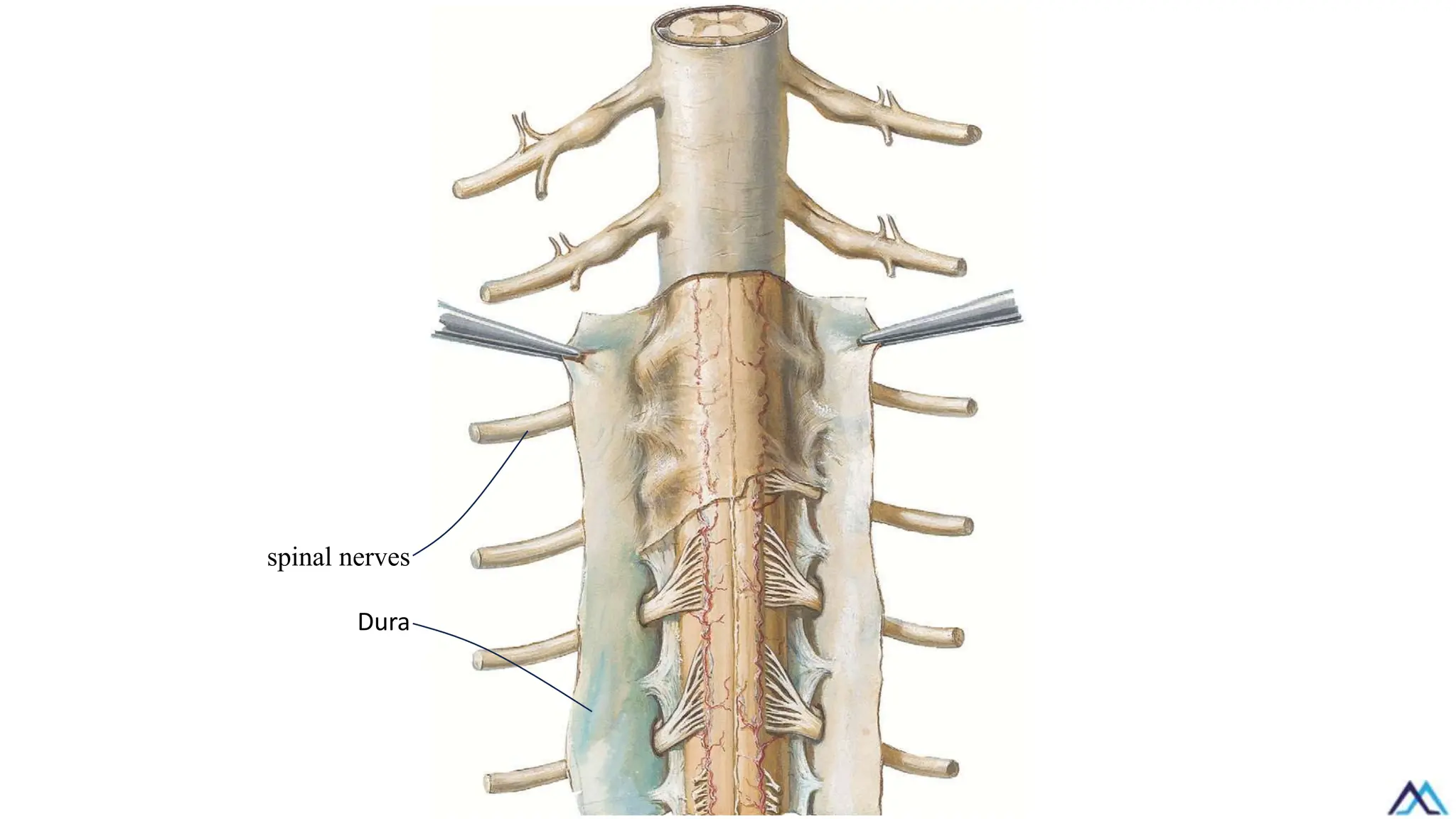
✓ It isthe outer & hardest layer
✓ Above, it is attached to the
foramen magnum and it is
continuing with the cerebral dura
✓ Throughout its length, it sends out
sleeves around the' trunks of the
spinal nerves
✓ Below, it extends beyond the
lower end of spinal cord (L1/L2),
it is attached to the 2nd sacral
vertebra.
1
2
3
5
4
S1
S2
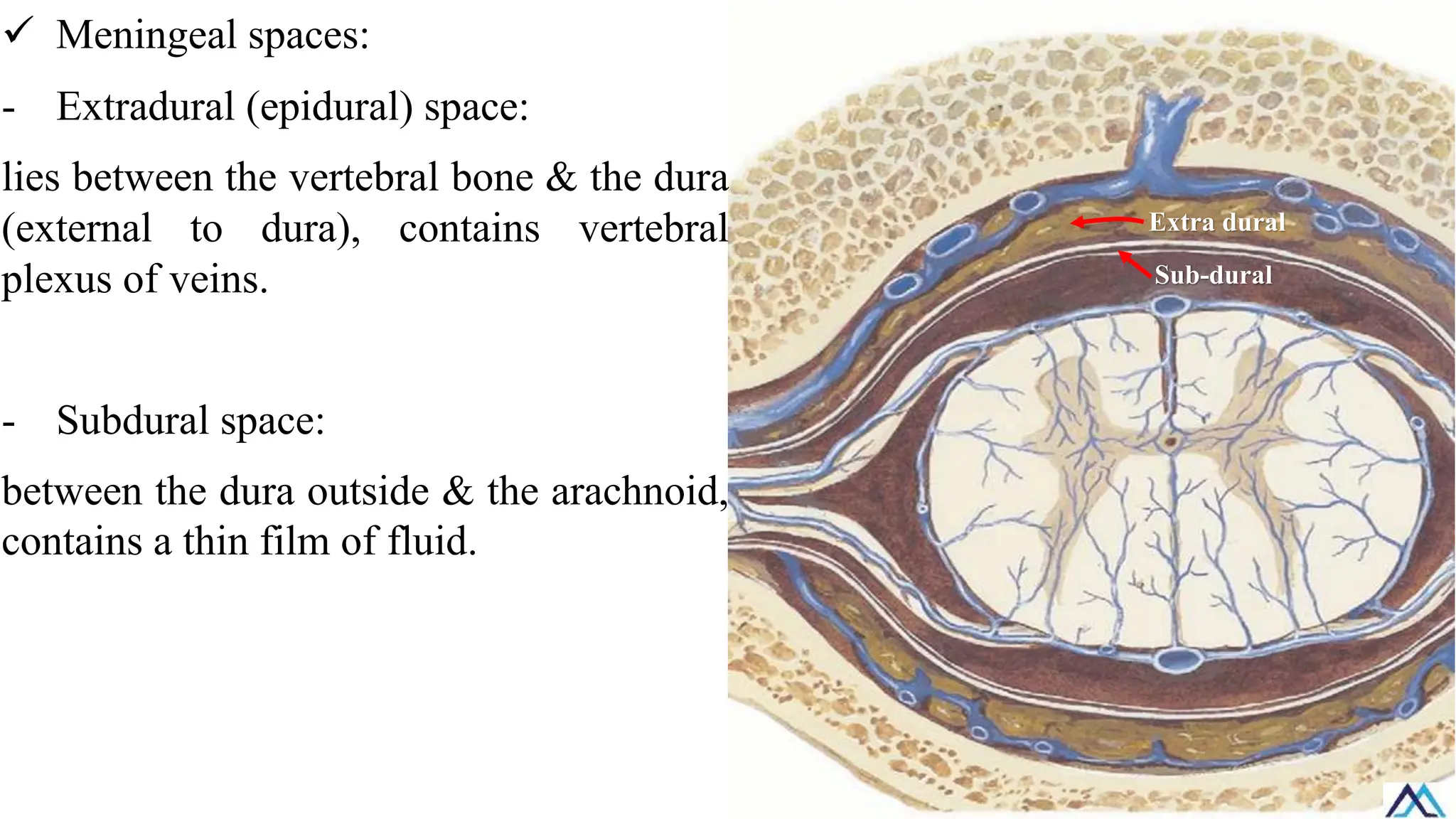
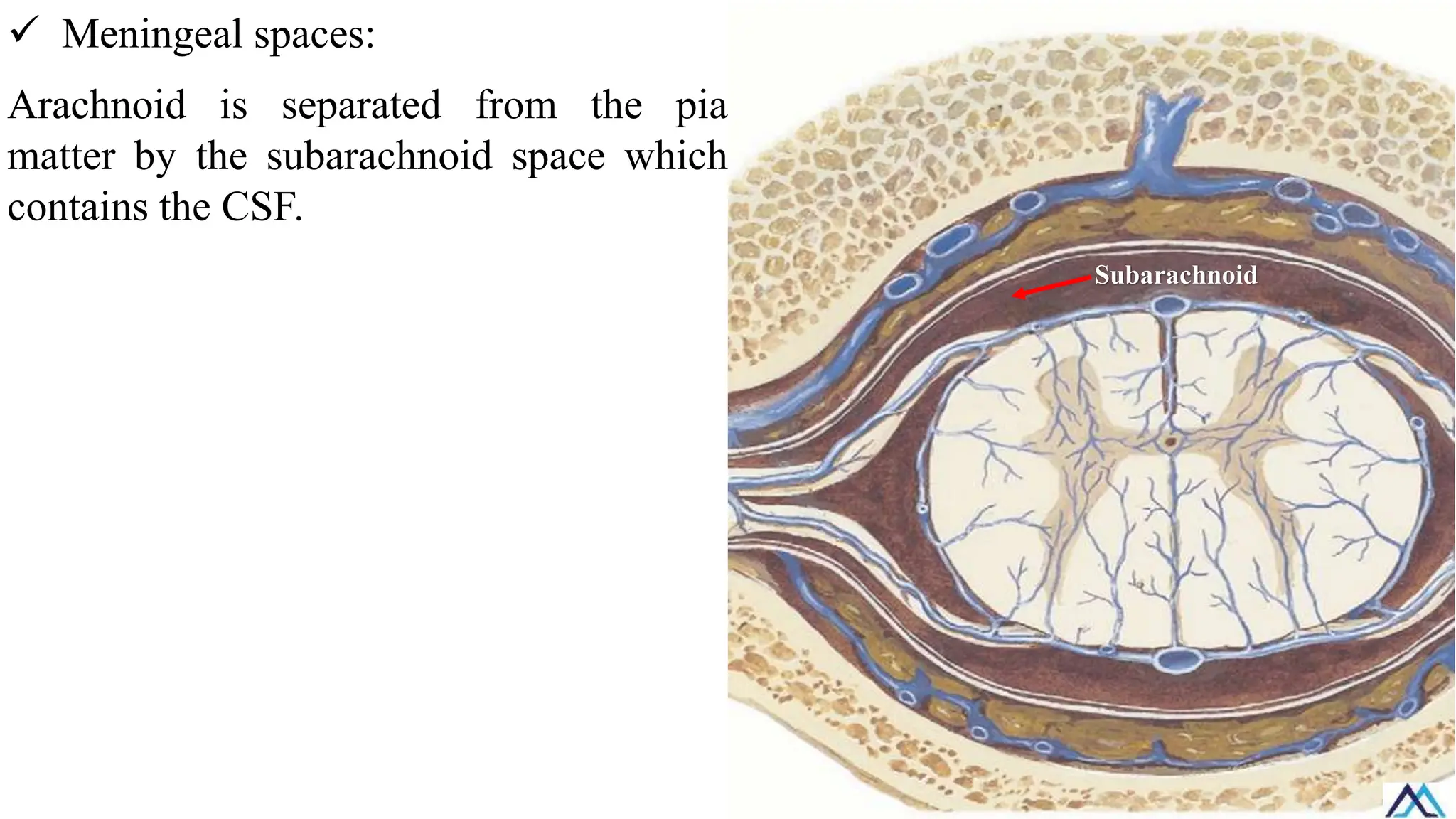
✓ Meningeal spaces:
-Extradural (epidural) space:
lies between the vertebral bone & the dura
(external to dura), contains vertebral
plexus of veins.
- Subdural space:
between the dura outside & the arachnoid,
contains a thin film of fluid.
Extra dural
Sub-dural
19.
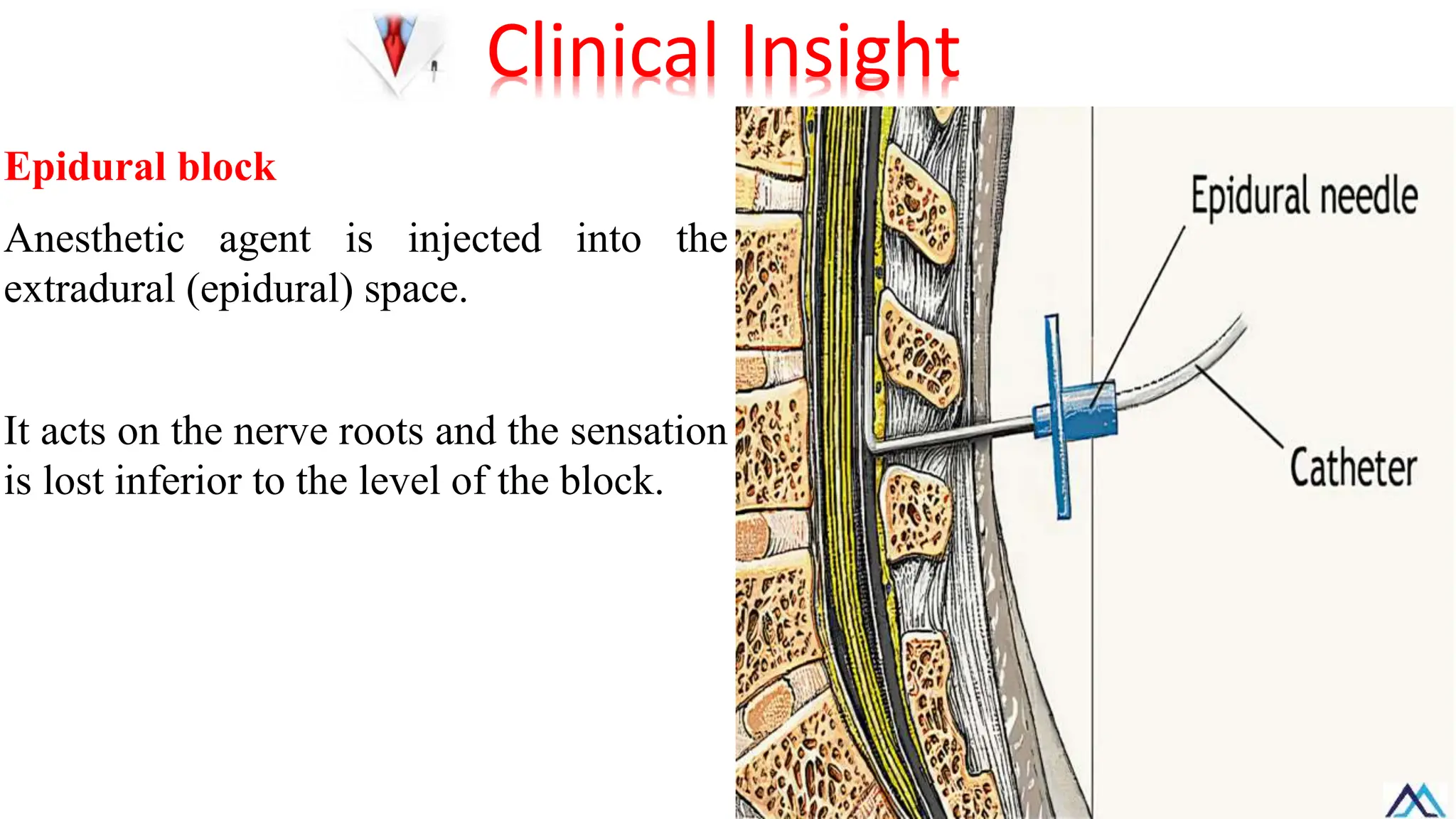
Epidural block
Anesthetic agentis injected into the
extradural (epidural) space.
It acts on the nerve roots and the sensation
is lost inferior to the level of the block.
Clinical Insight
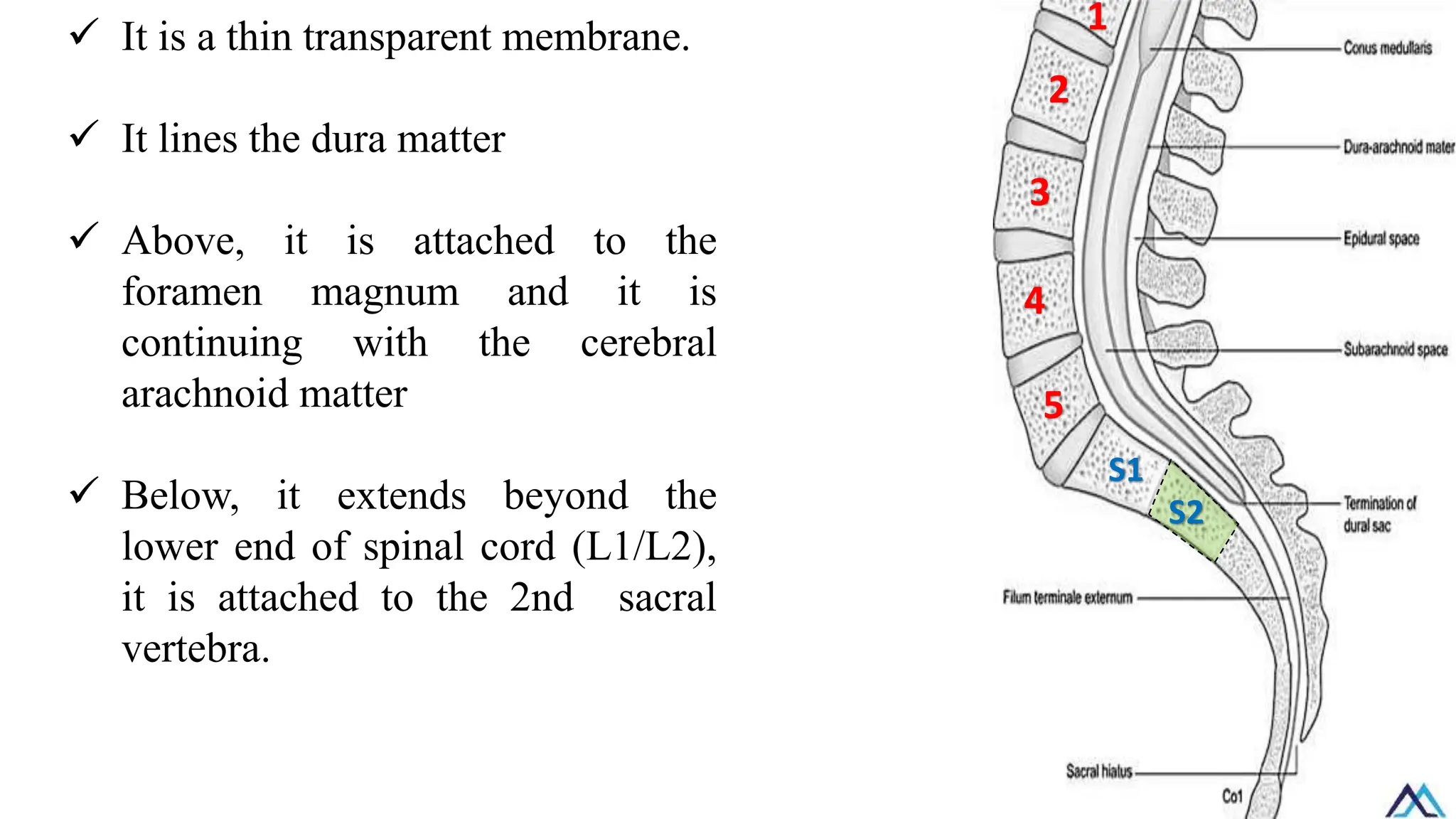
✓ It isa thin transparent membrane.
✓ It lines the dura matter
✓ Above, it is attached to the
foramen magnum and it is
continuing with the cerebral
arachnoid matter
✓ Below, it extends beyond the
lower end of spinal cord (L1/L2),
it is attached to the 2nd sacral
vertebra.
1
2
3
5
4
S1
S2
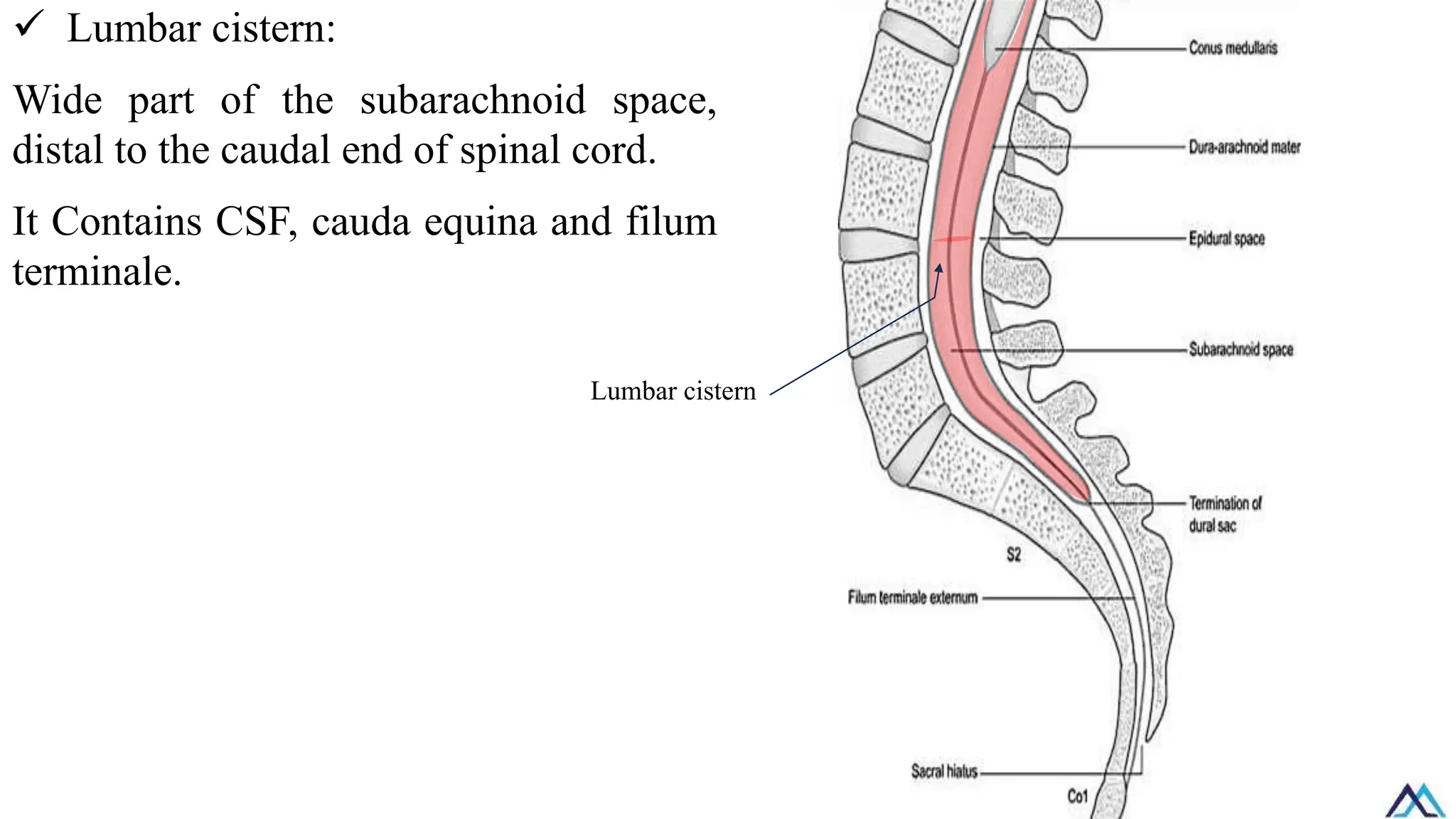
✓ Lumbar cistern:
Widepart of the subarachnoid space,
distal to the caudal end of spinal cord.
It Contains CSF, cauda equina and filum
terminale.
Lumbar cistern
26.
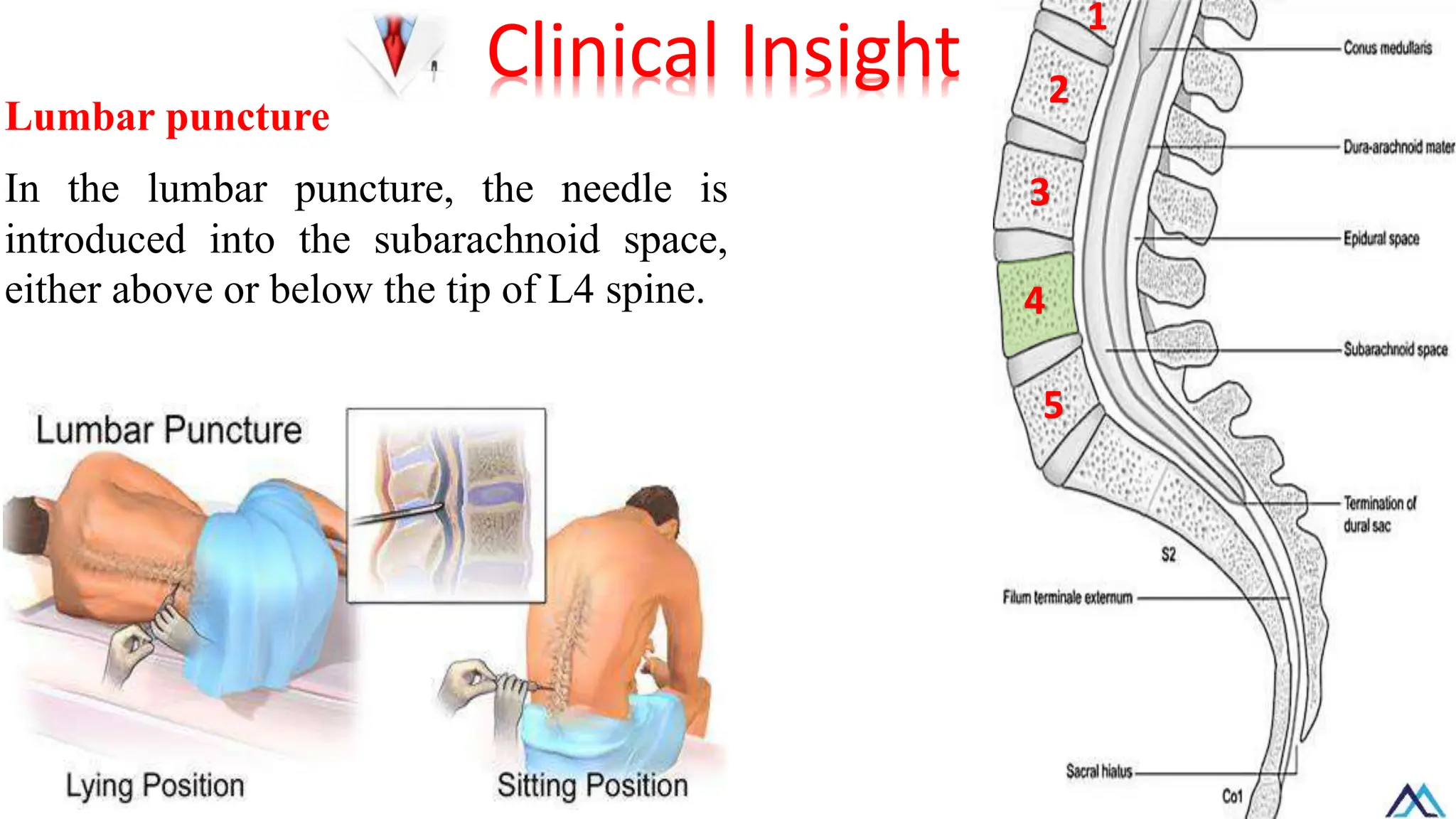
Lumbar puncture
In thelumbar puncture, the needle is
introduced into the subarachnoid space,
either above or below the tip of L4 spine.
Clinical Insight
1
2
3
5
4
27.
Lumbar puncture
• Diagnosticuses:
Obtaining C.S.F sample for analysis.
• Therapeutic uses:
Injection of local anesthetics and antibiotics.
C.S.F withdrawal to decrease intra-cranial pressure.
Clinical Insight
28.
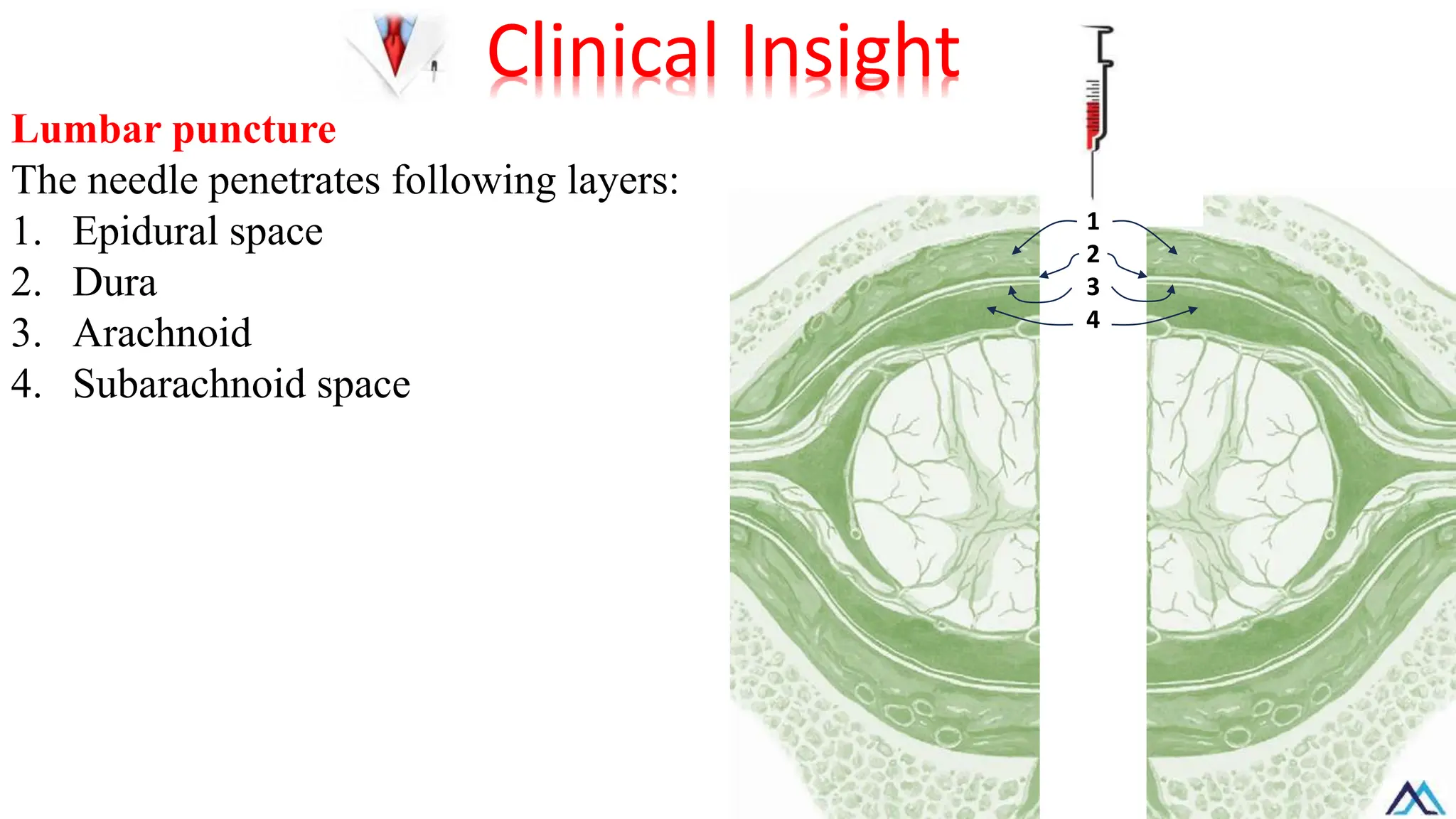
Lumbar puncture
The needlepenetrates following layers:
1. Epidural space
2. Dura
3. Arachnoid
4. Subarachnoid space
Clinical Insight
1
2
3
4
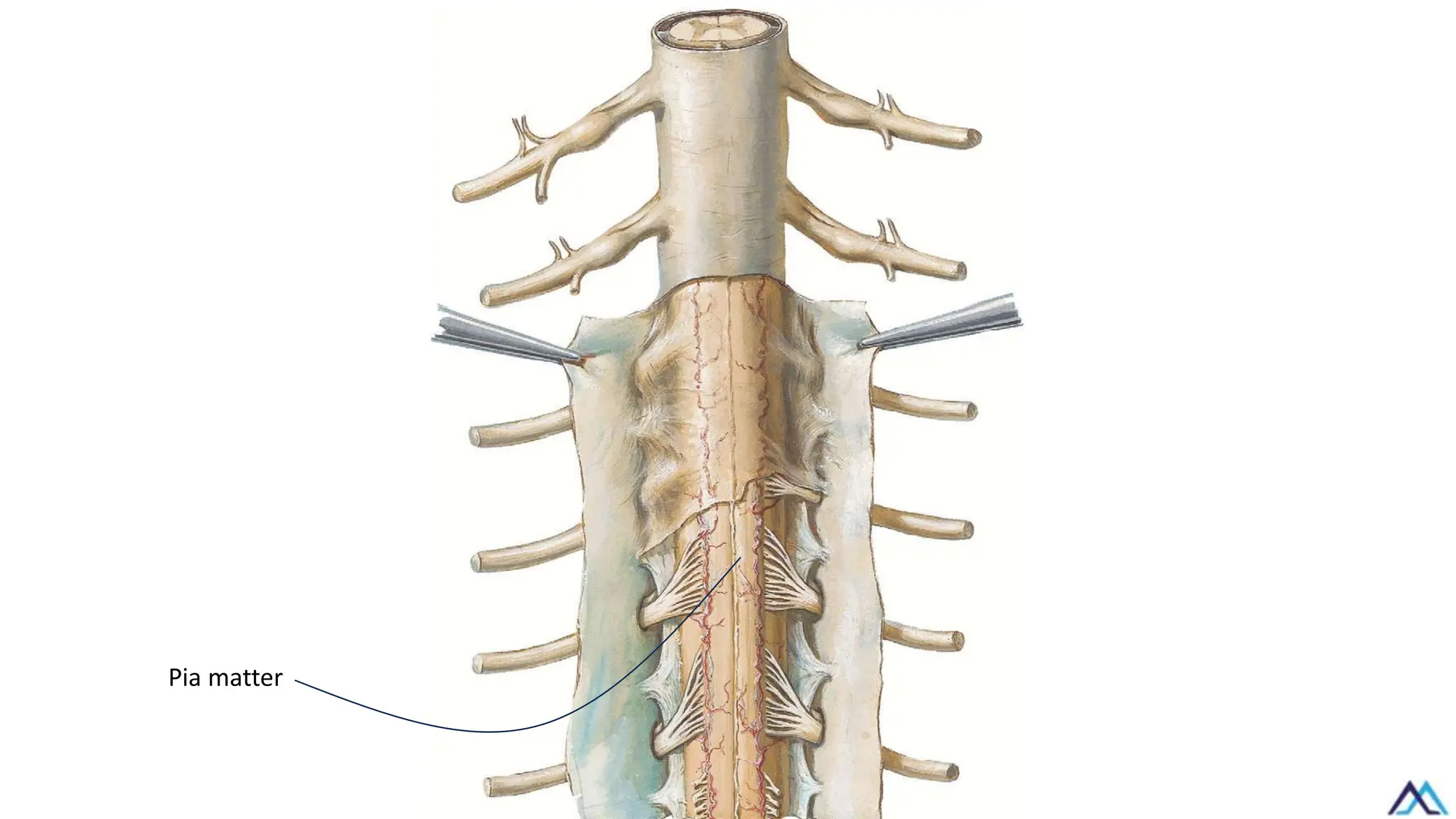
✓ It isa thin membrane firmly
adherent to the spinal cord.
✓ Above, it is continuous with the
pia matter of the brain.
✓ Below, it extends from the lower
tip of spinal cord (L1/L2), to form
the filum terminal which is
attached inferiorly to the back of
the coccyx.
1
2
3
5
4
Coccyx
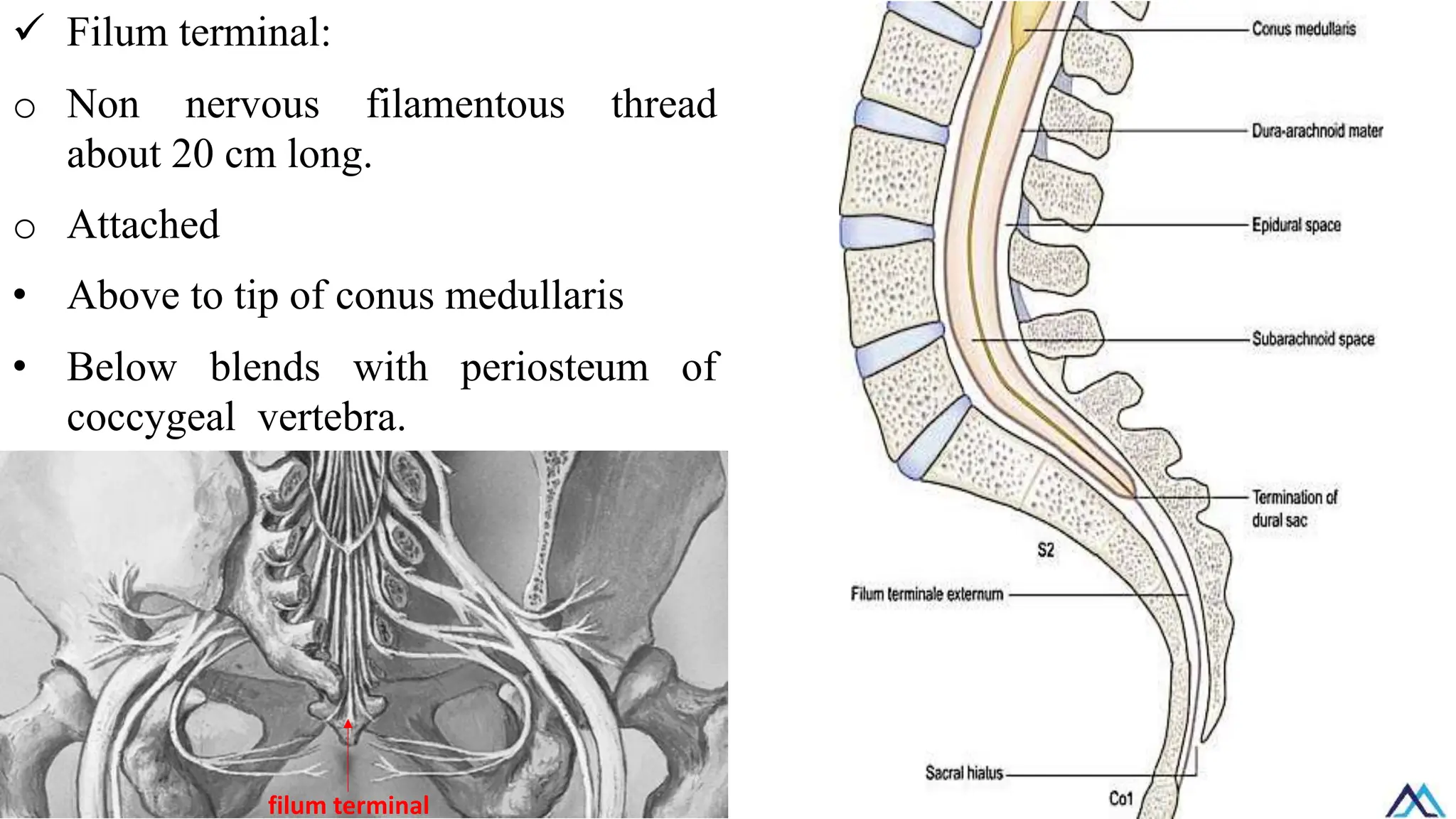
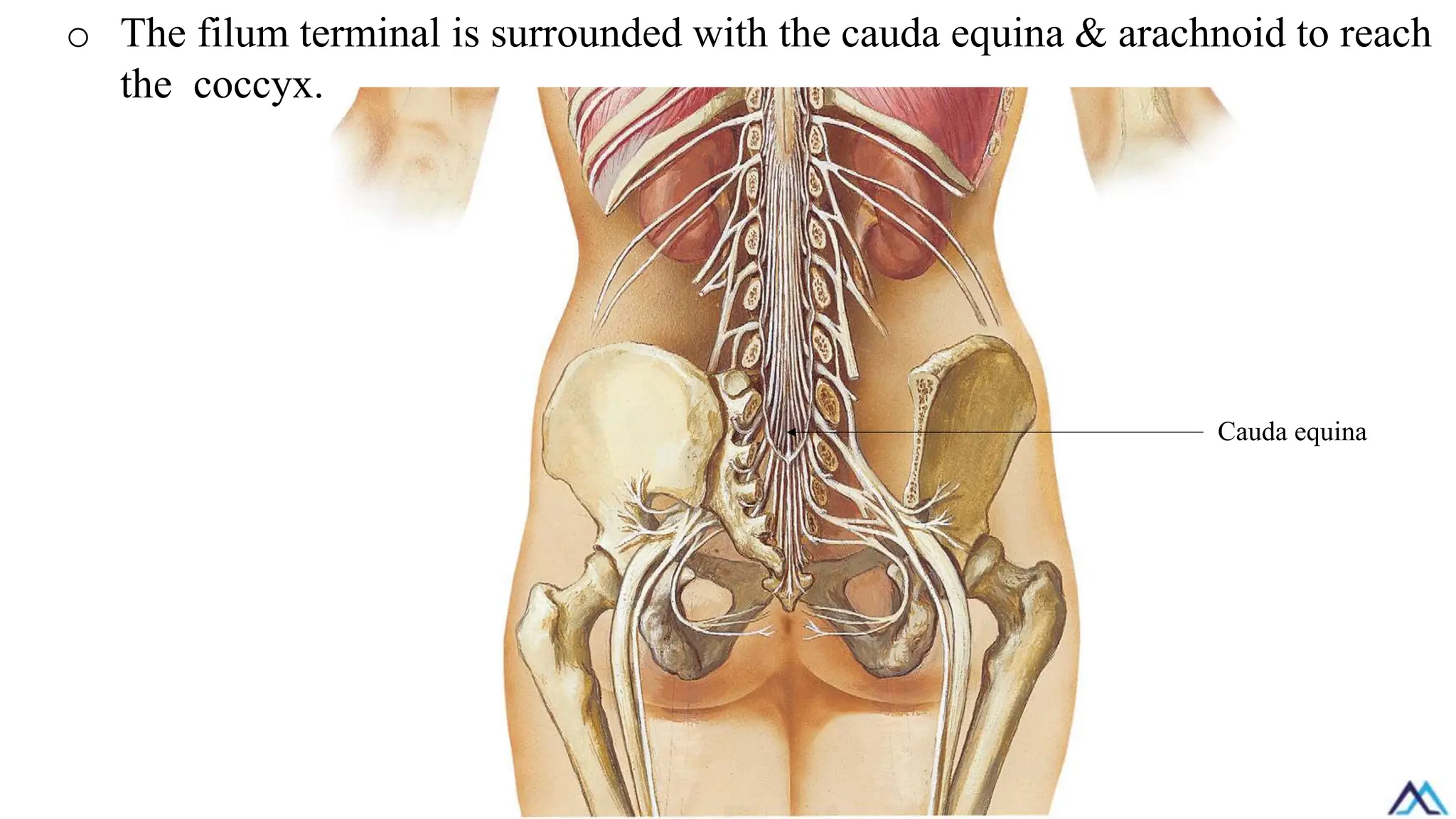
✓ Filum terminal:
oNon nervous filamentous thread
about 20 cm long.
o Attached
• Above to tip of conus medullaris
• Below blends with periosteum of
coccygeal vertebra.
filum terminal
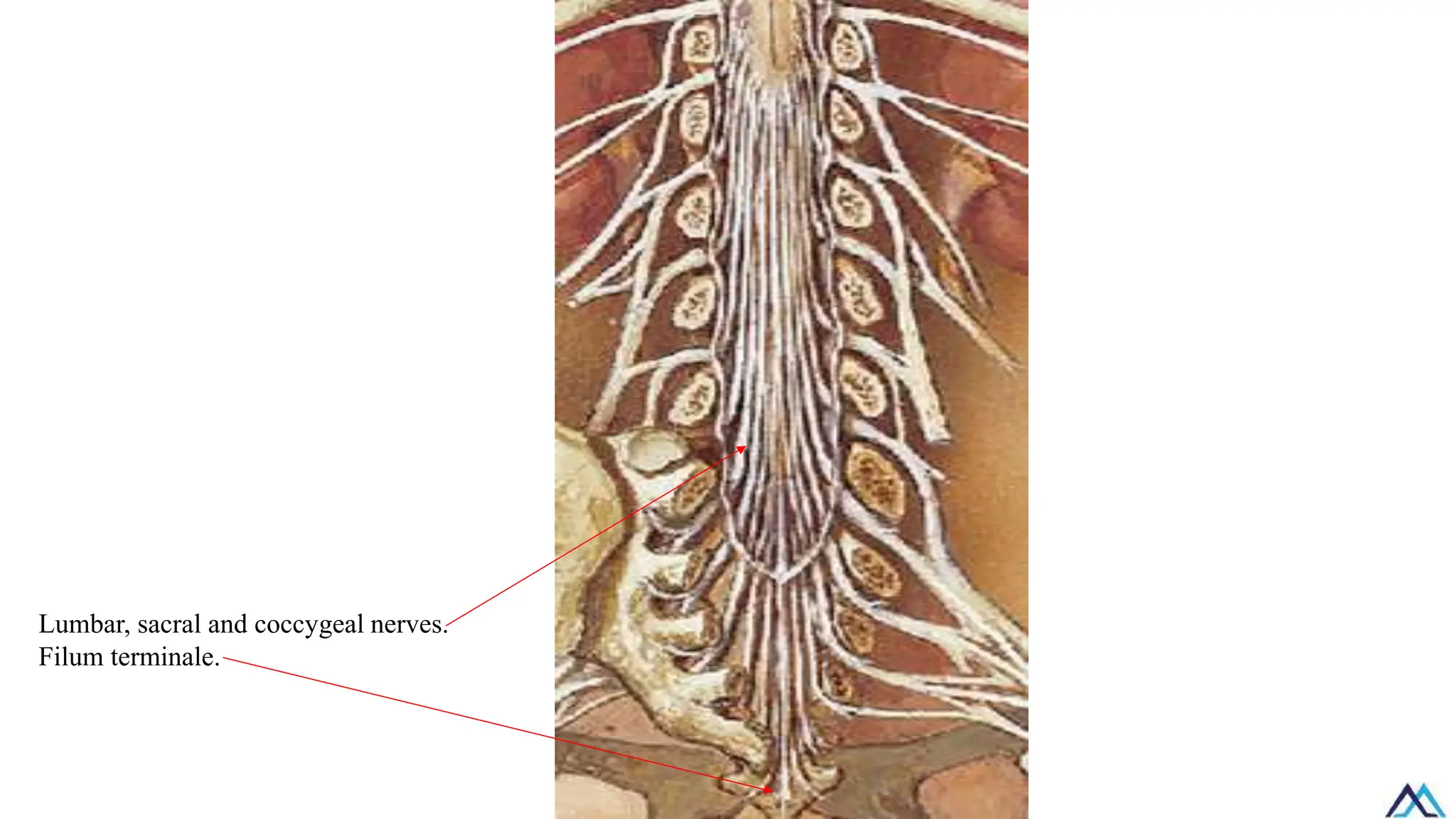
o The filumterminal is surrounded with the cauda equina & arachnoid to reach
the coccyx.
Cauda equina
35.
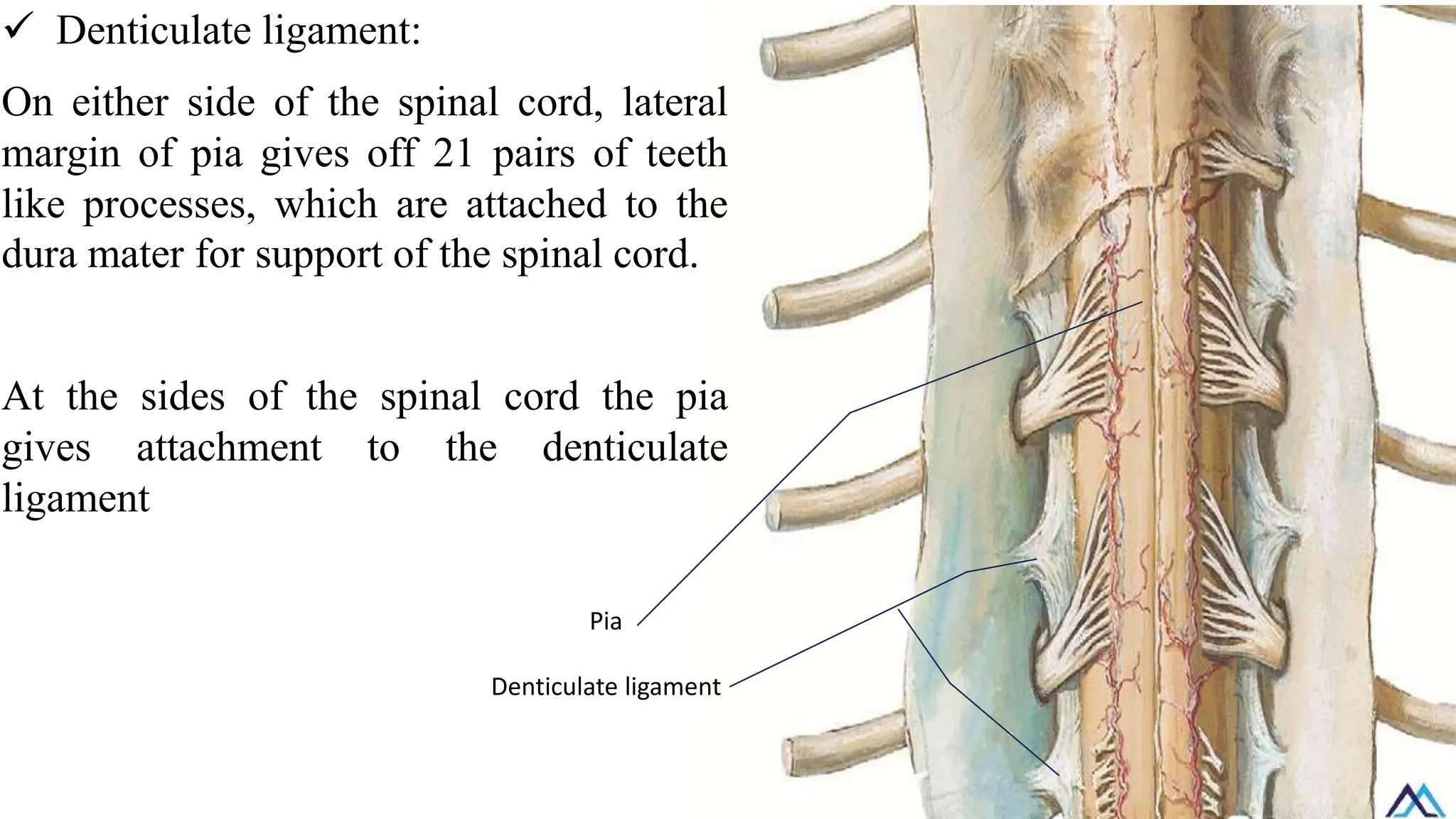
✓ Denticulate ligament:
Oneither side of the spinal cord, lateral
margin of pia gives off 21 pairs of teeth
like processes, which are attached to the
dura mater for support of the spinal cord.
At the sides of the spinal cord the pia
gives attachment to the denticulate
ligament
Pia
Denticulate ligament
36.
B- Meninges ofthe brain
Dura matter
Arachnoid matter
Pia matter
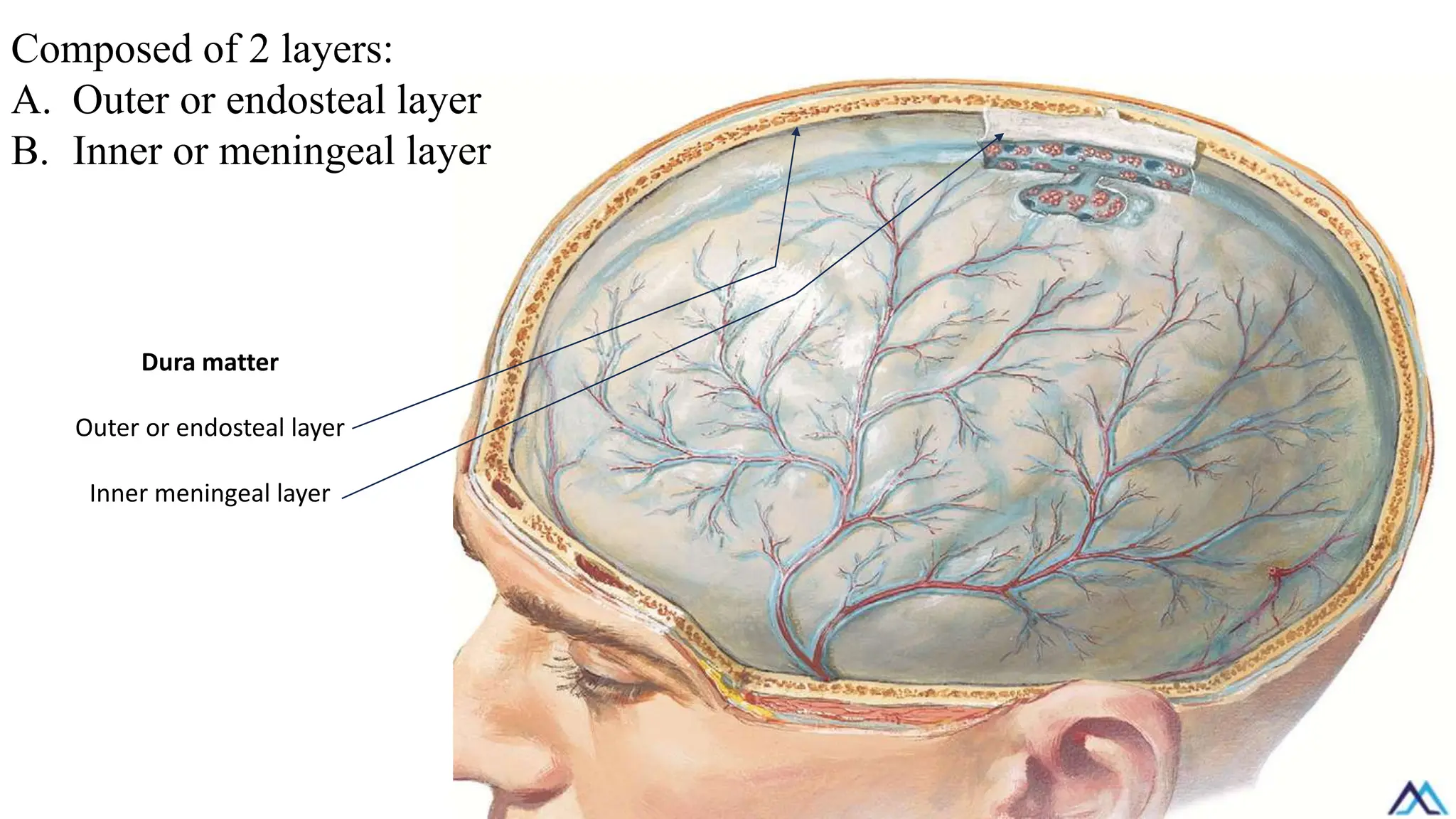
Composed of 2layers:
A. Outer or endosteal layer
B. Inner or meningeal layer
Dura matter
Outer or endosteal layer
Inner meningeal layer
39.
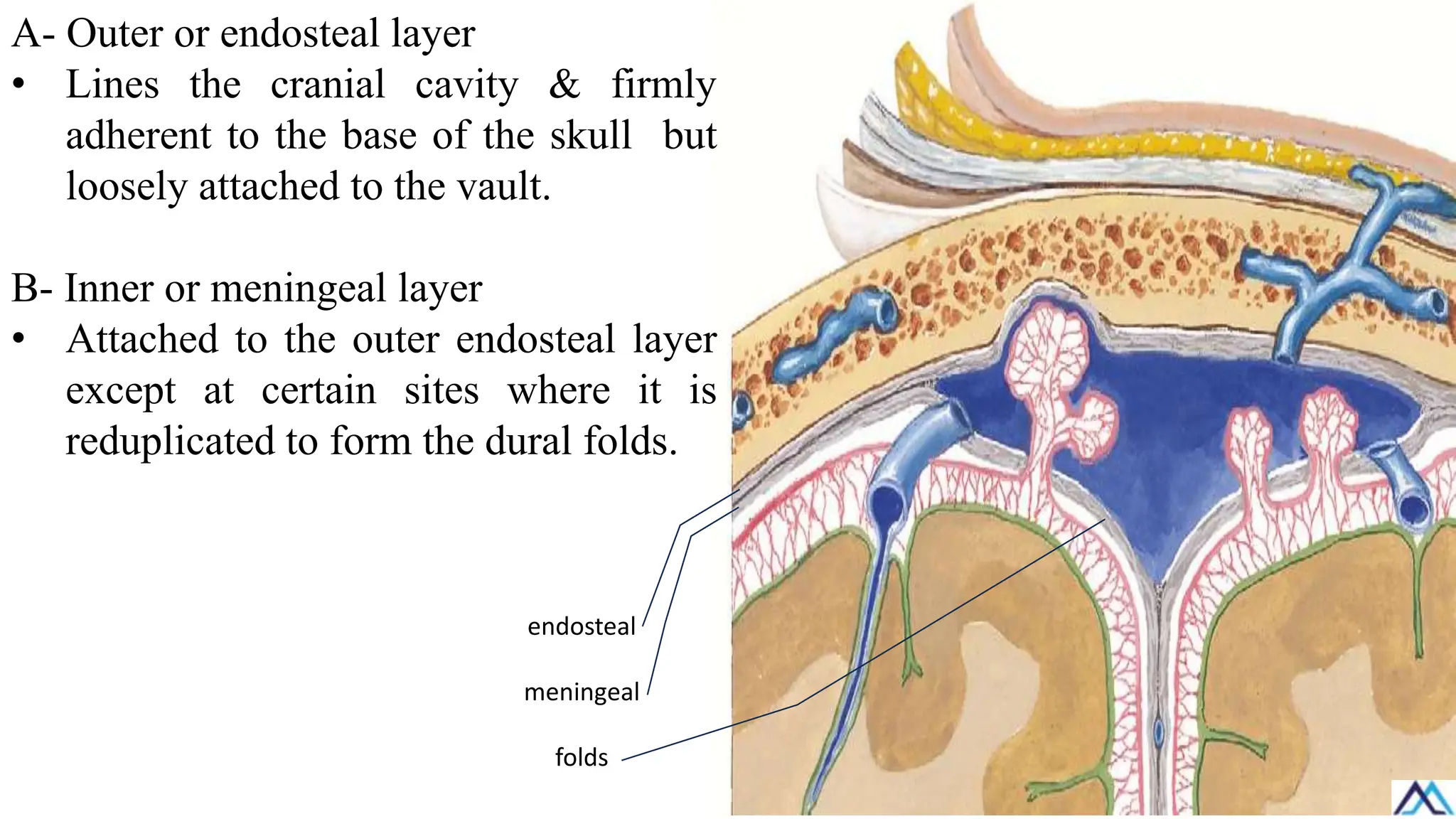
A- Outer orendosteal layer
• Lines the cranial cavity & firmly
adherent to the base of the skull but
loosely attached to the vault.
B- Inner or meningeal layer
• Attached to the outer endosteal layer
except at certain sites where it is
reduplicated to form the dural folds.
endosteal
meningeal
folds
40.
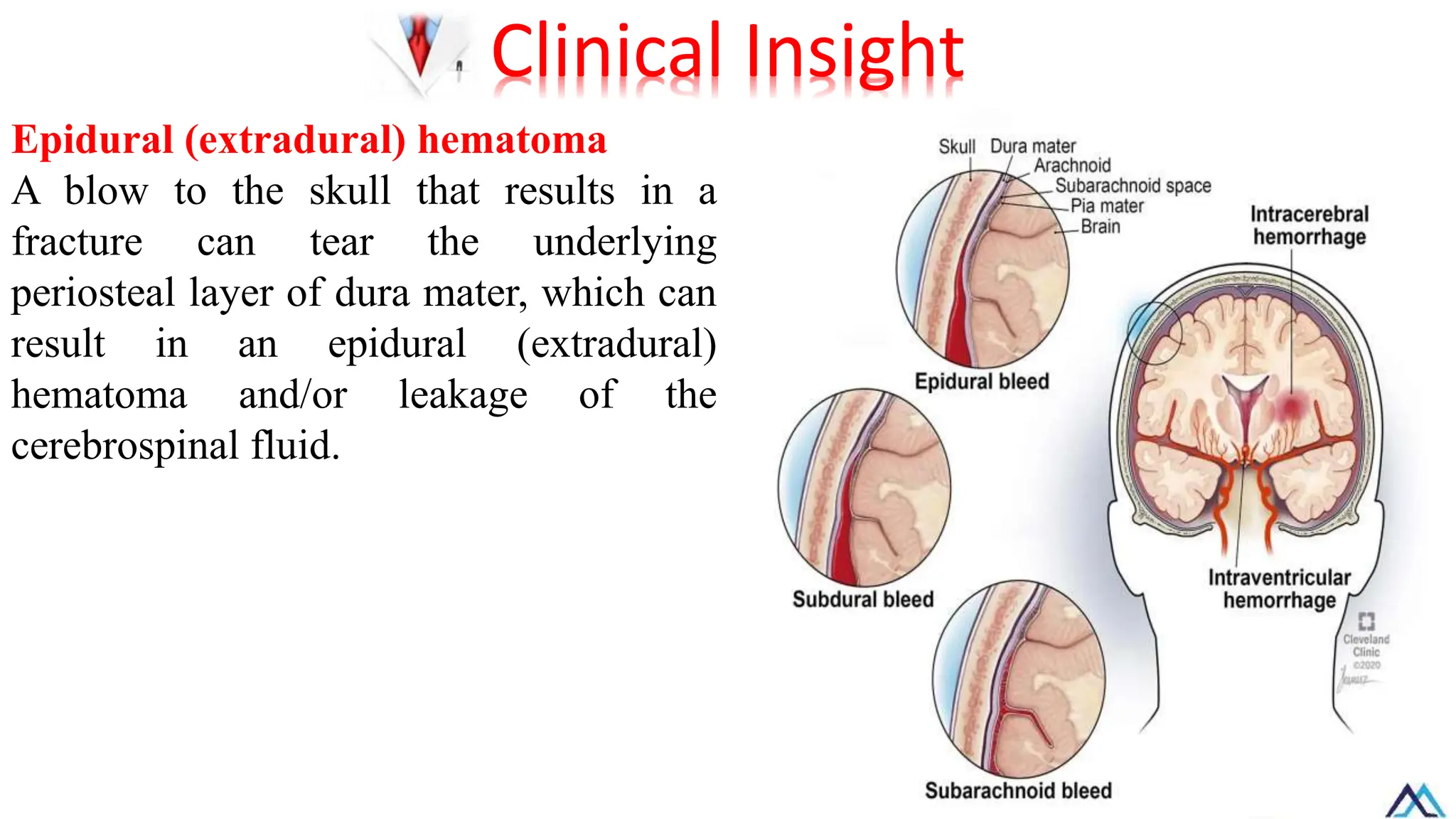
Epidural (extradural) hematoma
Ablow to the skull that results in a
fracture can tear the underlying
periosteal layer of dura mater, which can
result in an epidural (extradural)
hematoma and/or leakage of the
cerebrospinal fluid.
Clinical Insight
41.
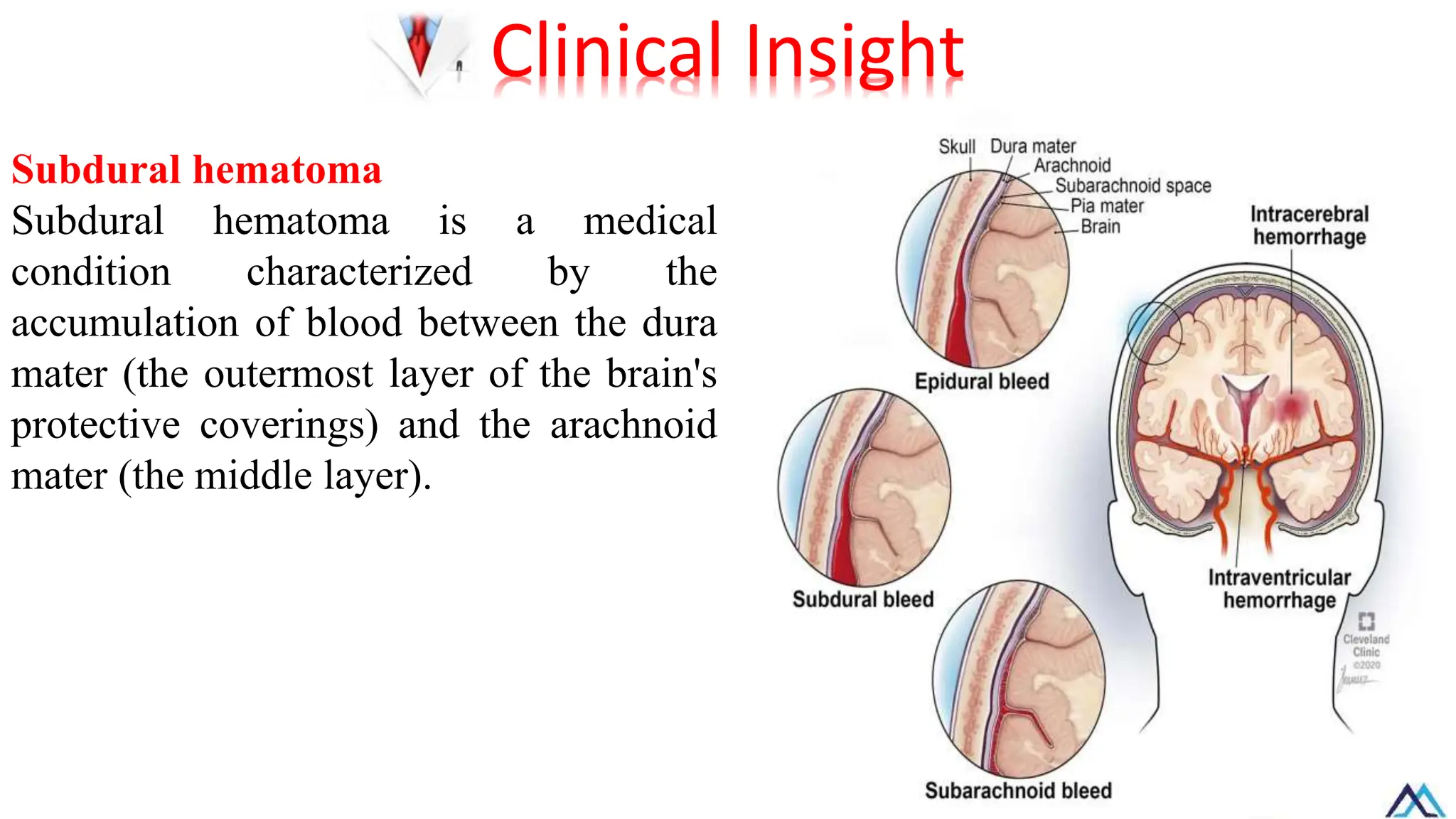
Subdural hematoma
Subdural hematomais a medical
condition characterized by the
accumulation of blood between the dura
mater (the outermost layer of the brain's
protective coverings) and the arachnoid
mater (the middle layer).
Clinical Insight
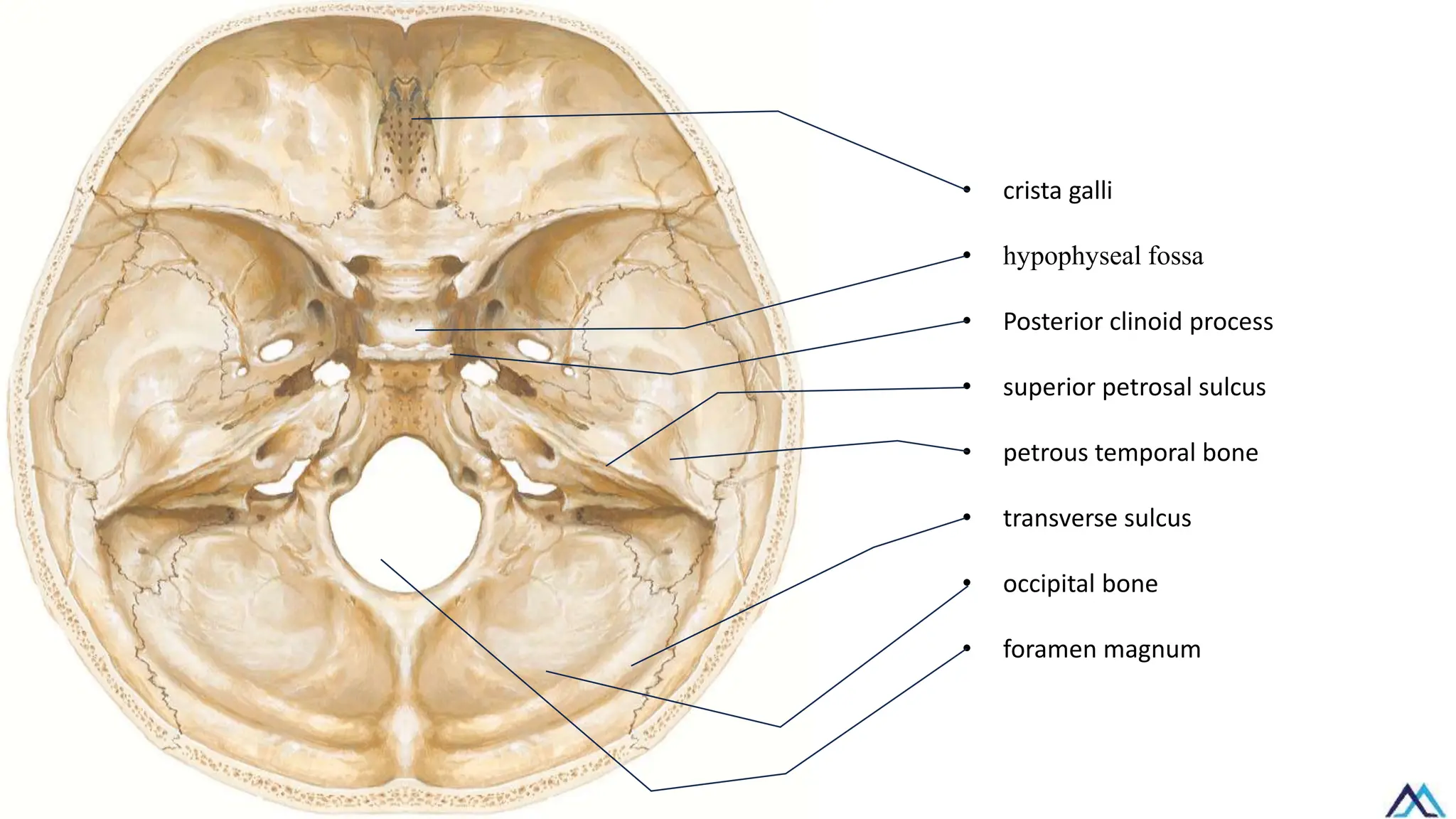
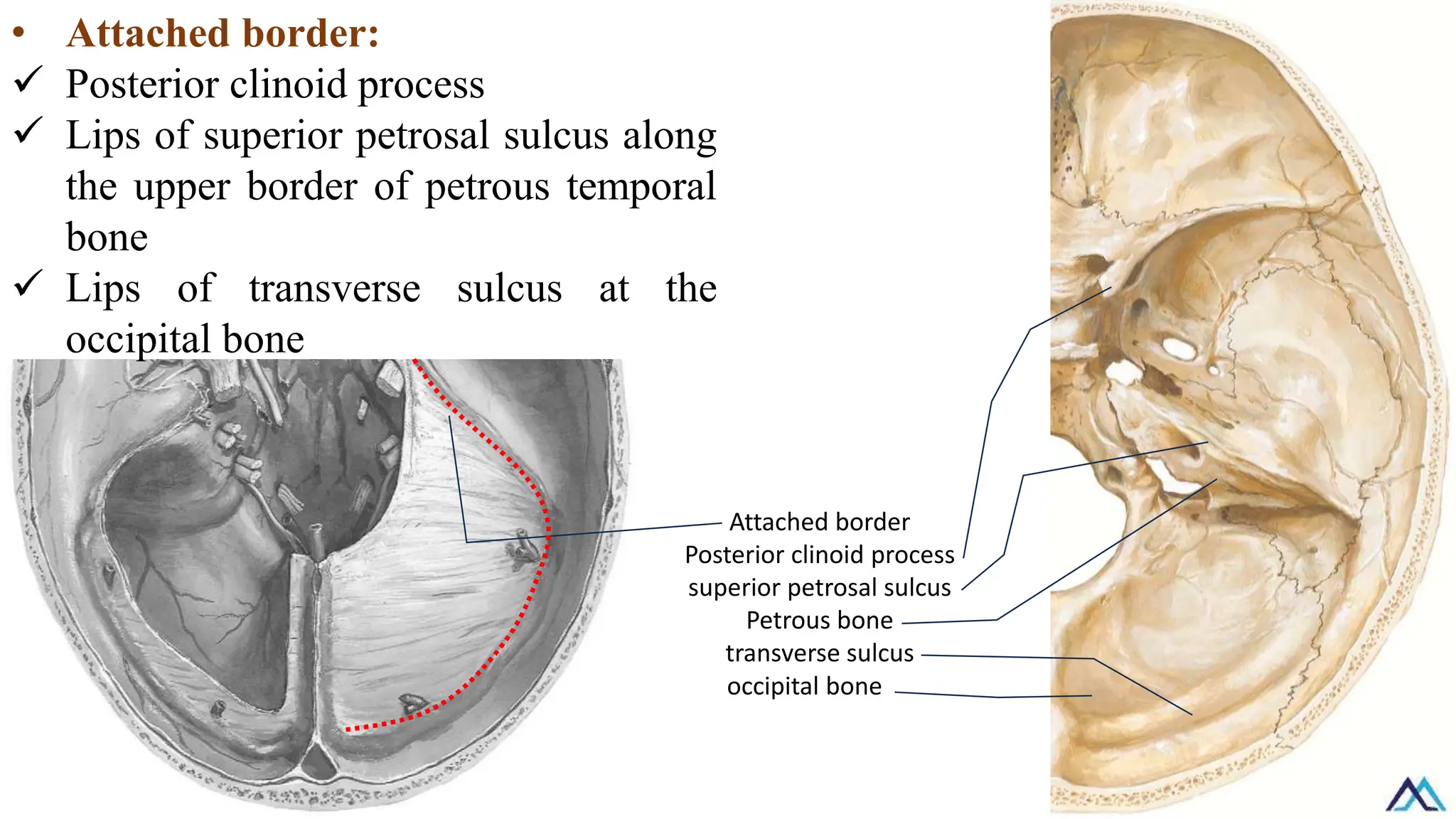
Attached border
Posterior clinoidprocess
superior petrosal sulcus
Petrous bone
transverse sulcus
occipital bone
• Attached border:
✓ Posterior clinoid process
✓ Lips of superior petrosal sulcus along
the upper border of petrous temporal
bone
✓ Lips of transverse sulcus at the
occipital bone
46.
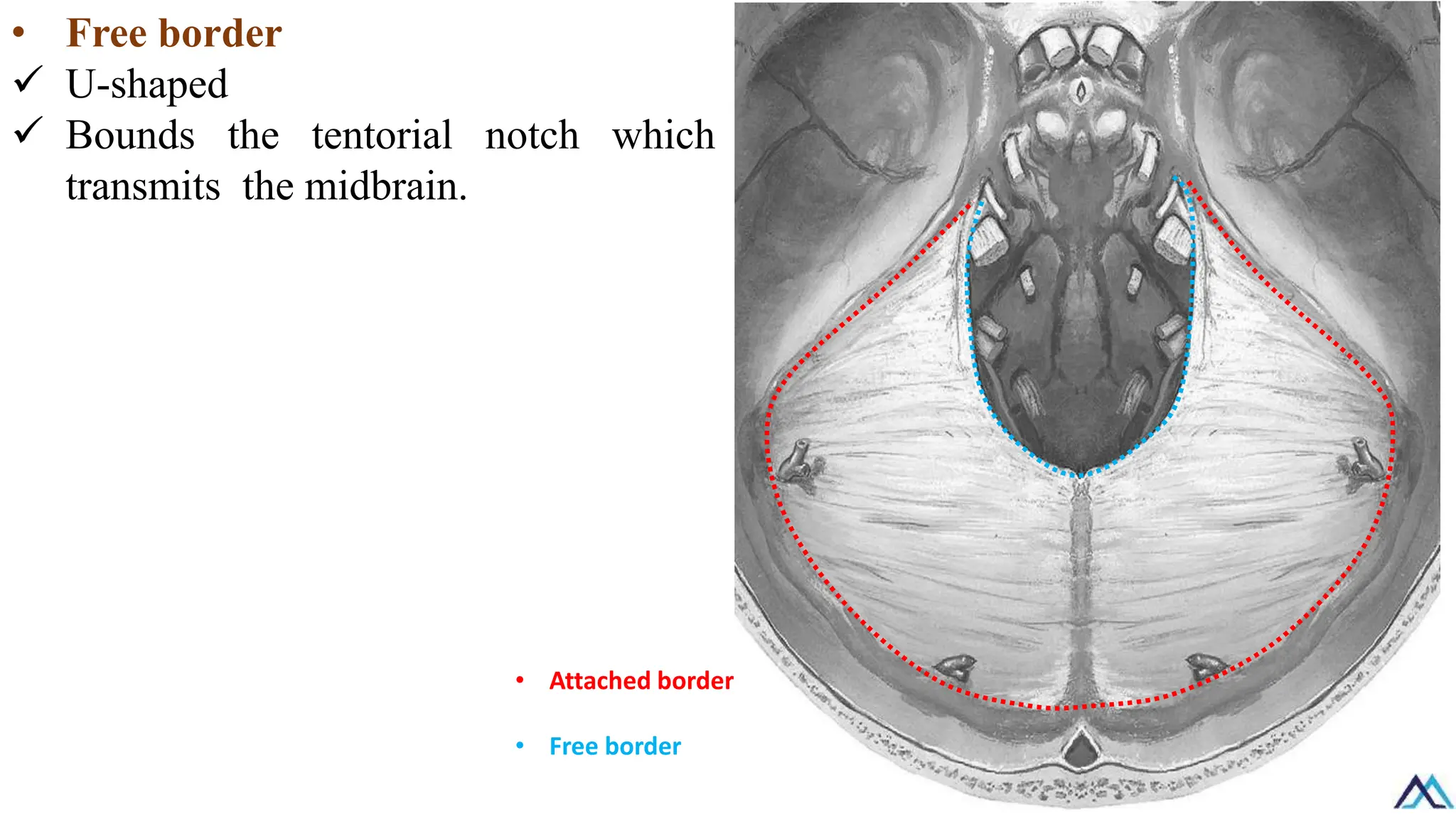
• Free border
✓U-shaped
✓ Bounds the tentorial notch which
transmits the midbrain.
• Attached border
• Free border
47.
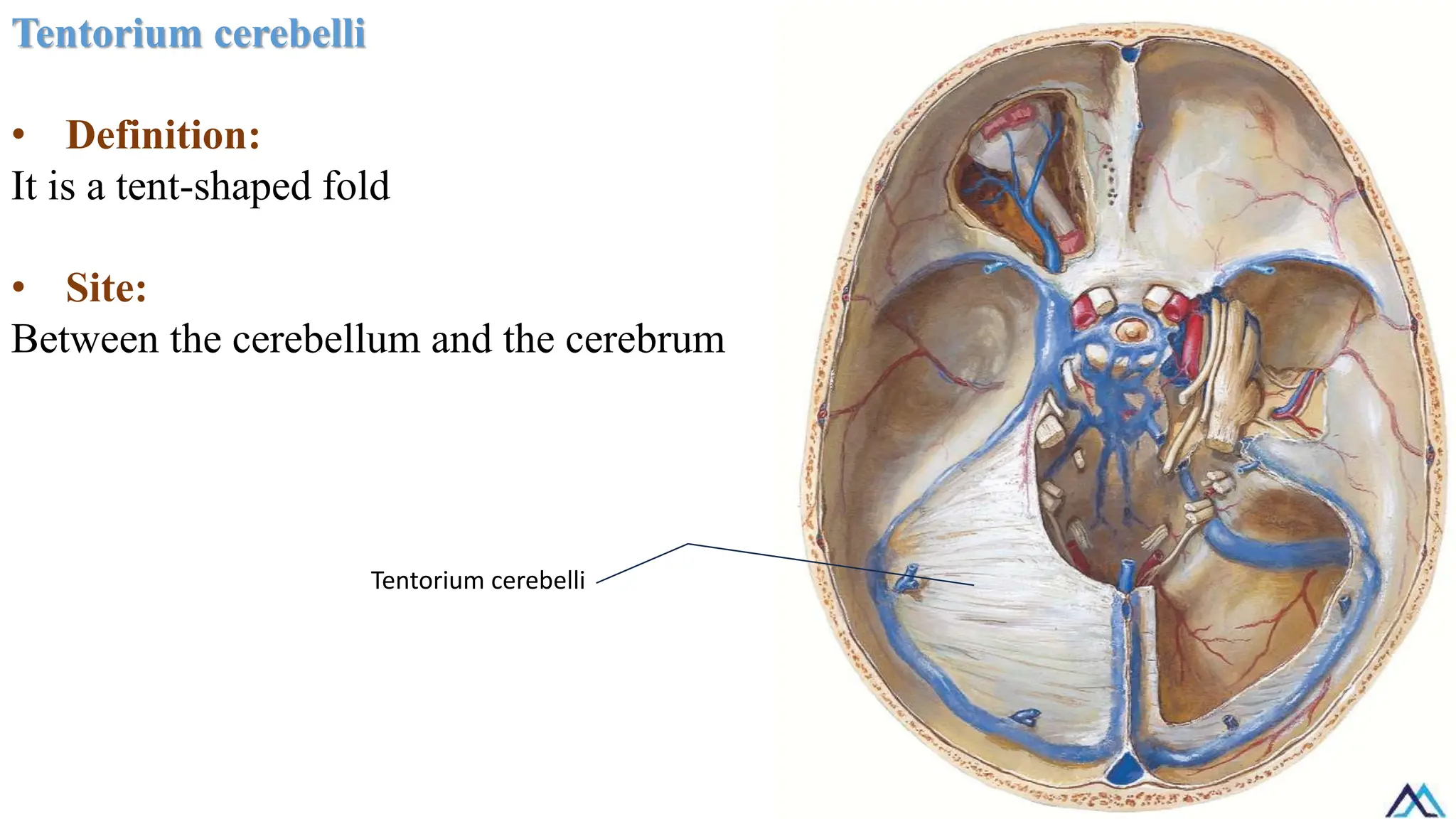
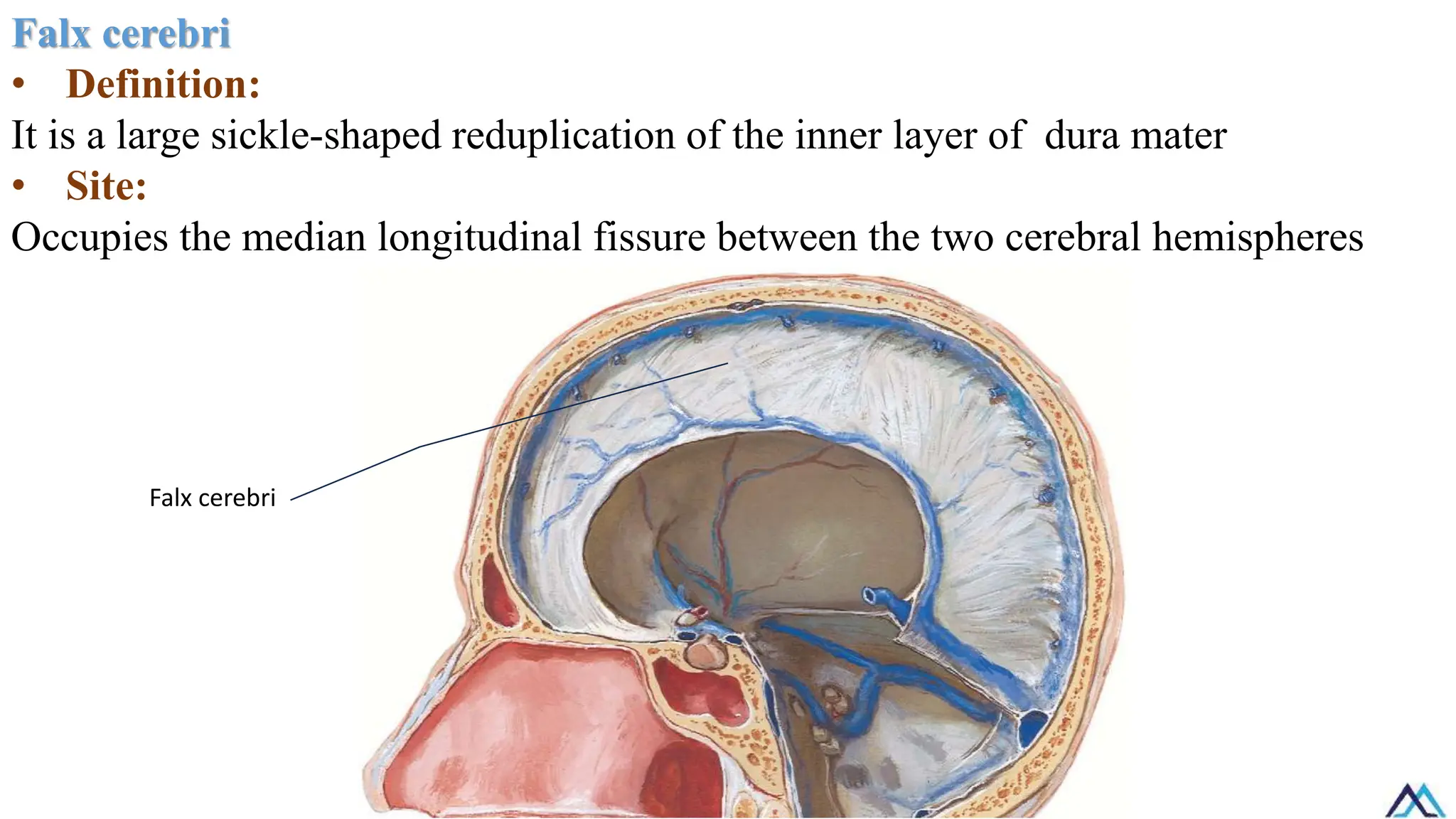
Falx cerebri
• Definition:
Itis a large sickle-shaped reduplication of the inner layer of dura mater
• Site:
Occupies the median longitudinal fissure between the two cerebral hemispheres
Falx cerebri
48.
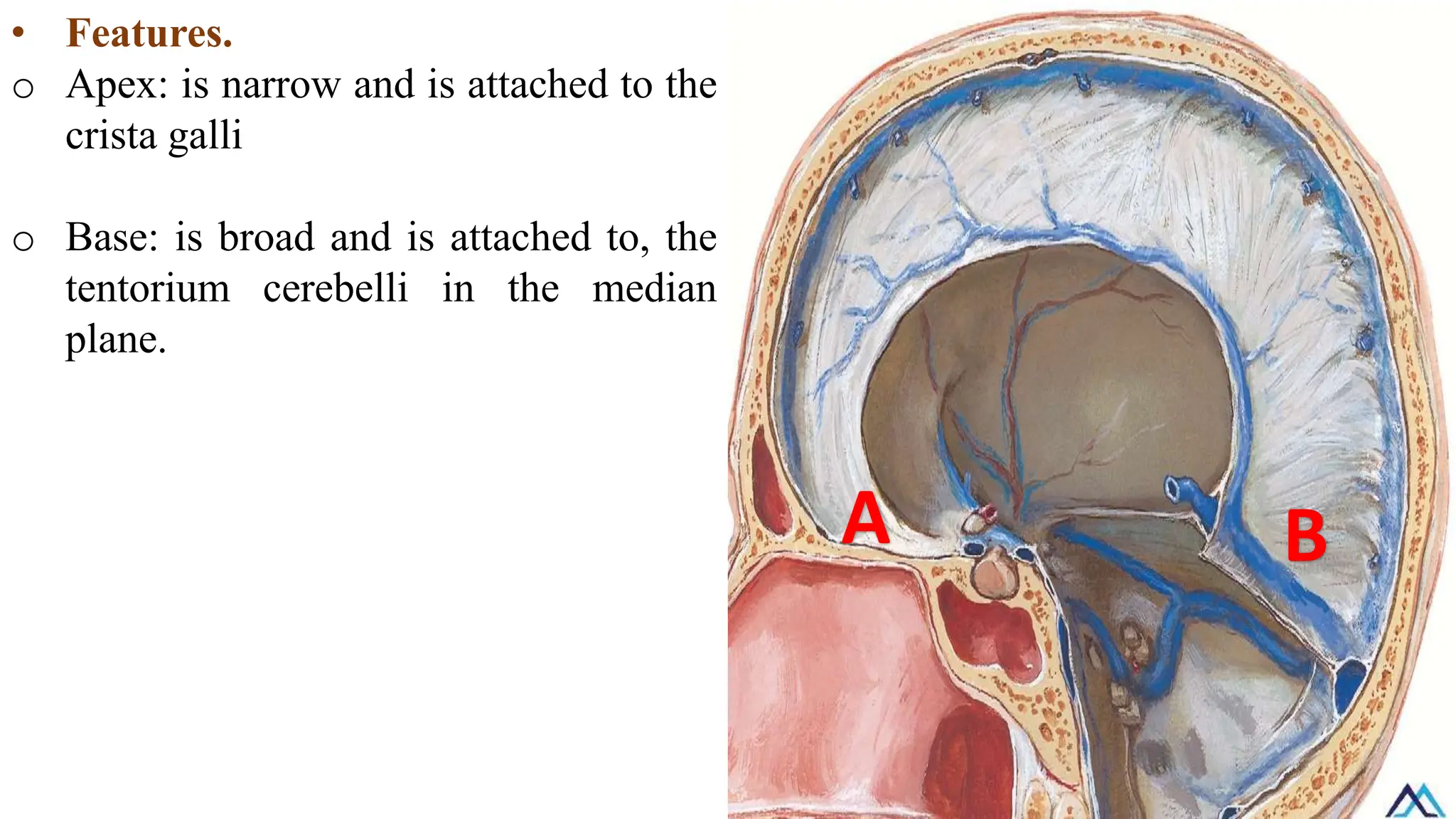
• Features.
o Apex:is narrow and is attached to the
crista galli
o Base: is broad and is attached to, the
tentorium cerebelli in the median
plane.
A B
49.
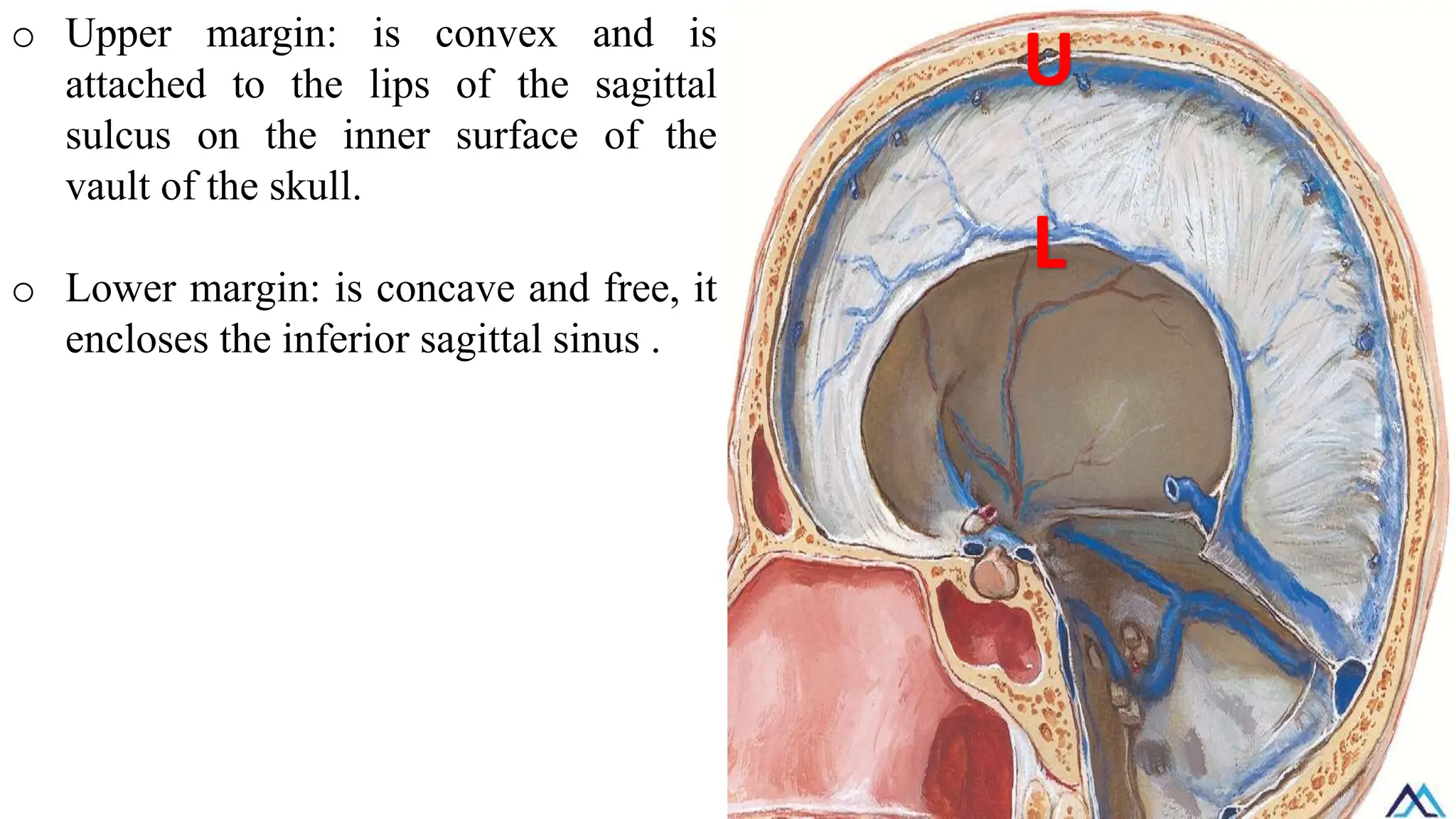
o Upper margin:is convex and is
attached to the lips of the sagittal
sulcus on the inner surface of the
vault of the skull.
o Lower margin: is concave and free, it
encloses the inferior sagittal sinus .
U
L
50.
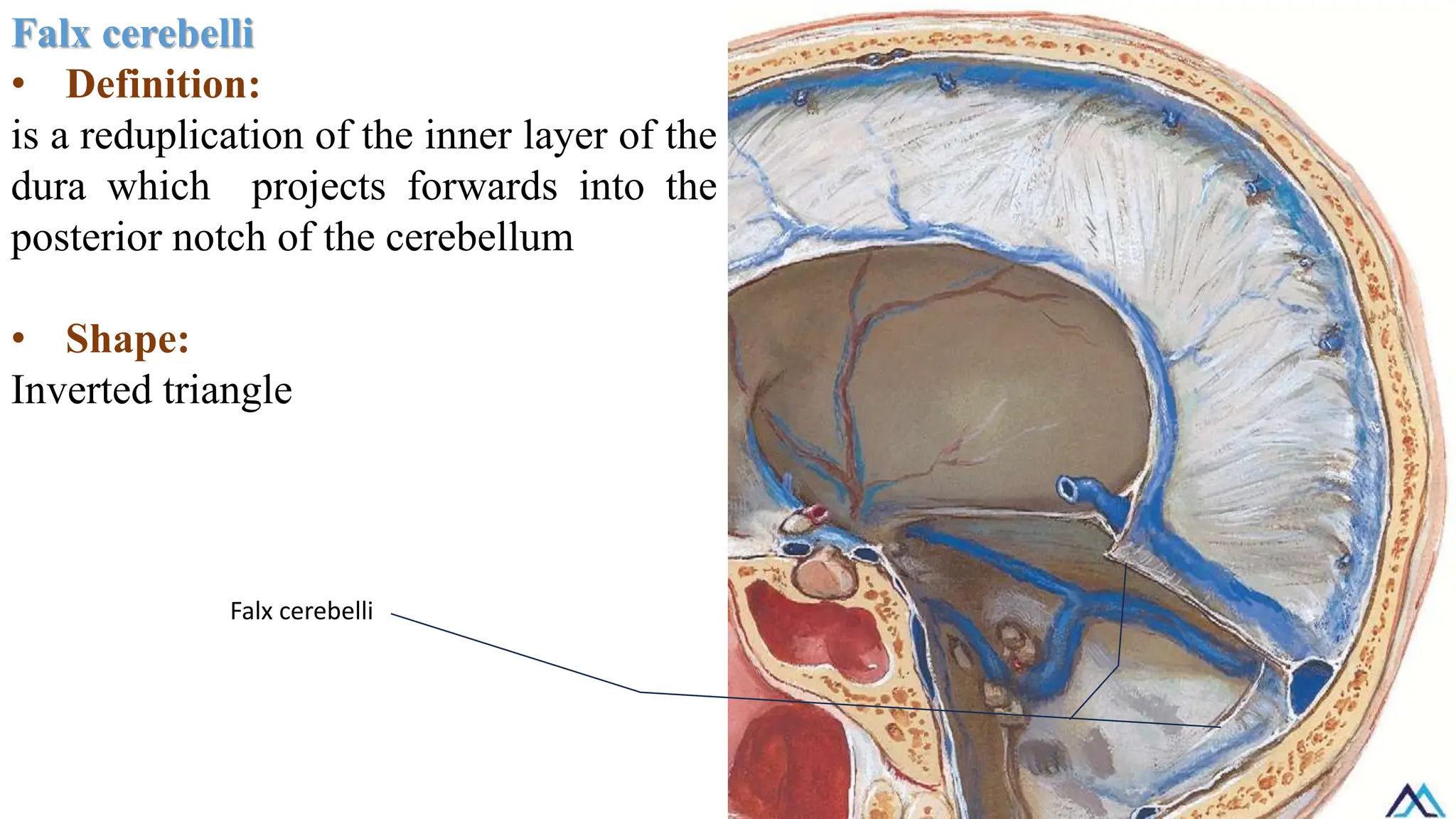
Falx cerebelli
• Definition:
isa reduplication of the inner layer of the
dura which projects forwards into the
posterior notch of the cerebellum
• Shape:
Inverted triangle
Falx cerebelli
51.
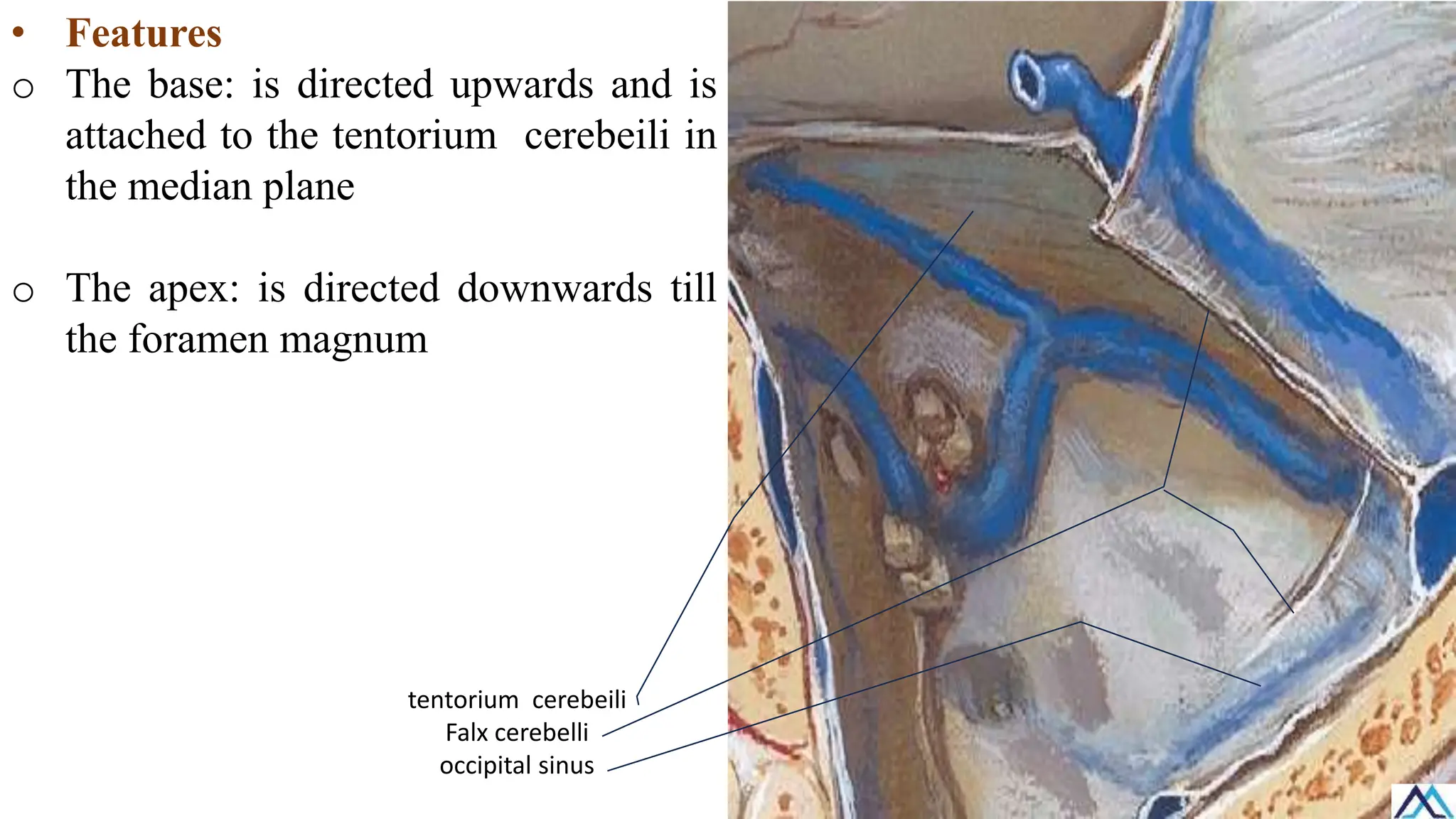
• Features
o Thebase: is directed upwards and is
attached to the tentorium cerebeili in
the median plane
o The apex: is directed downwards till
the foramen magnum
tentorium cerebeili
Falx cerebelli
occipital sinus
52.
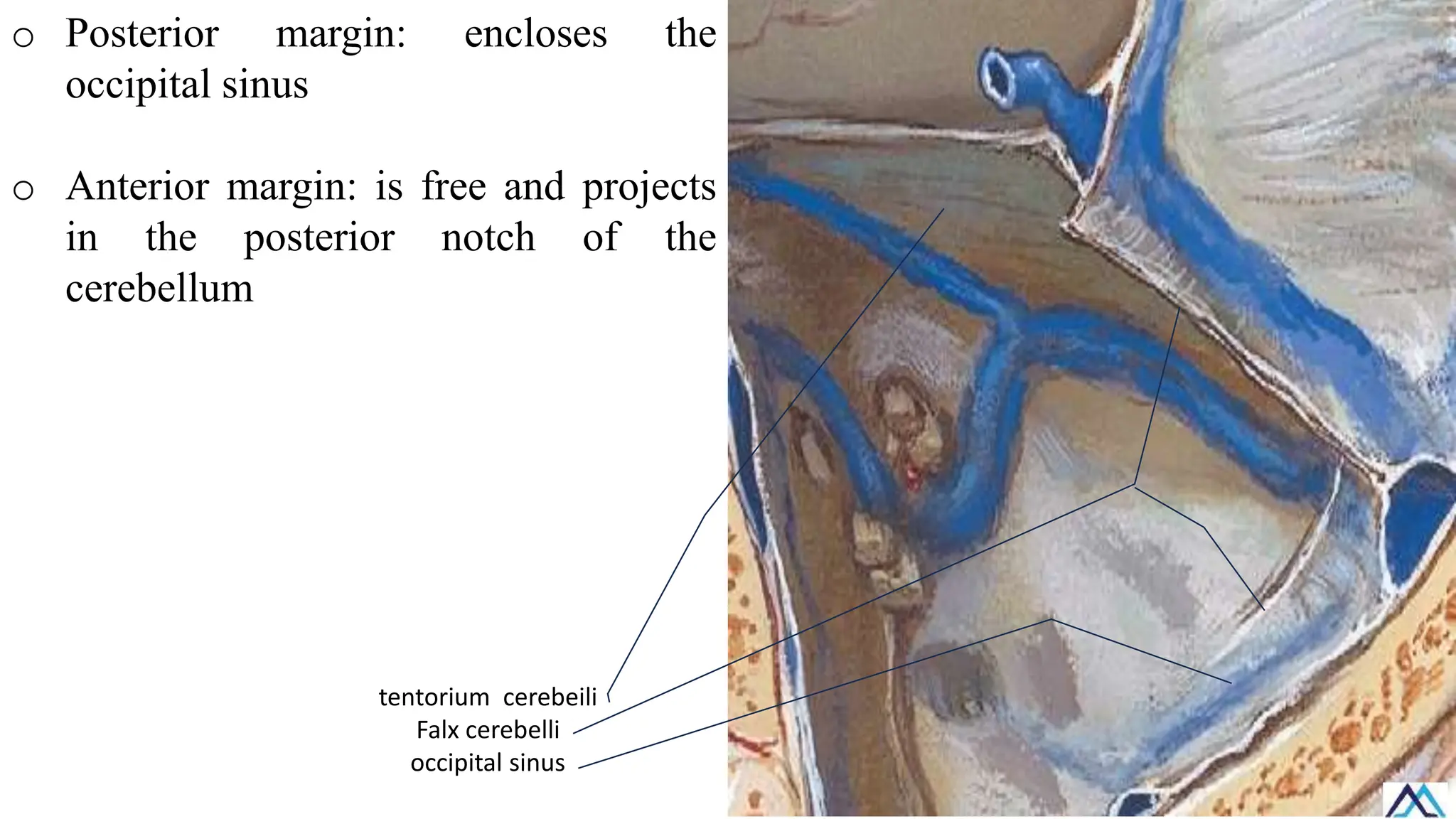
o Posterior margin:encloses the
occipital sinus
o Anterior margin: is free and projects
in the posterior notch of the
cerebellum
tentorium cerebeili
Falx cerebelli
occipital sinus
53.
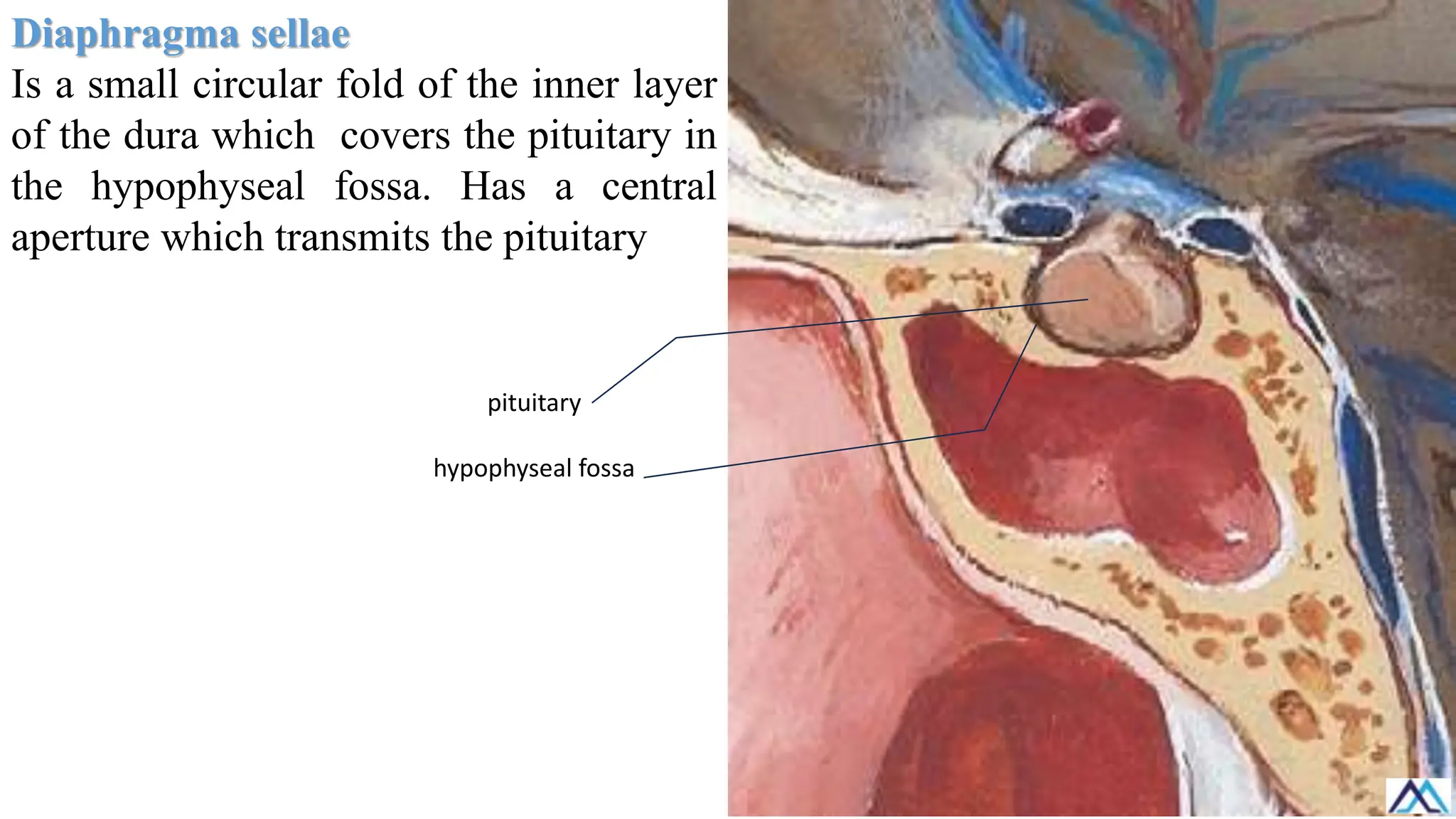
Diaphragma sellae
Is asmall circular fold of the inner layer
of the dura which covers the pituitary in
the hypophyseal fossa. Has a central
aperture which transmits the pituitary
pituitary
hypophyseal fossa
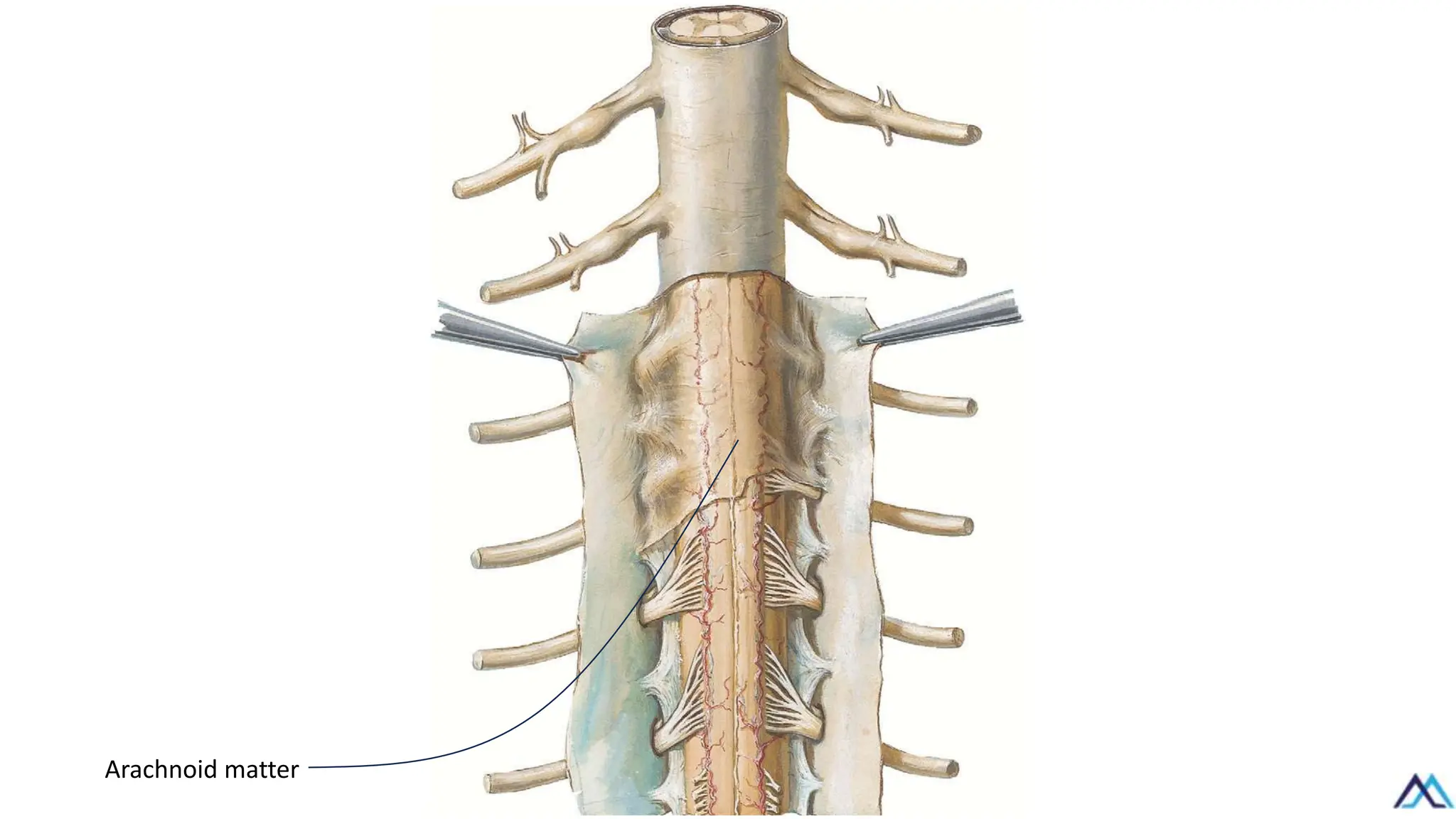
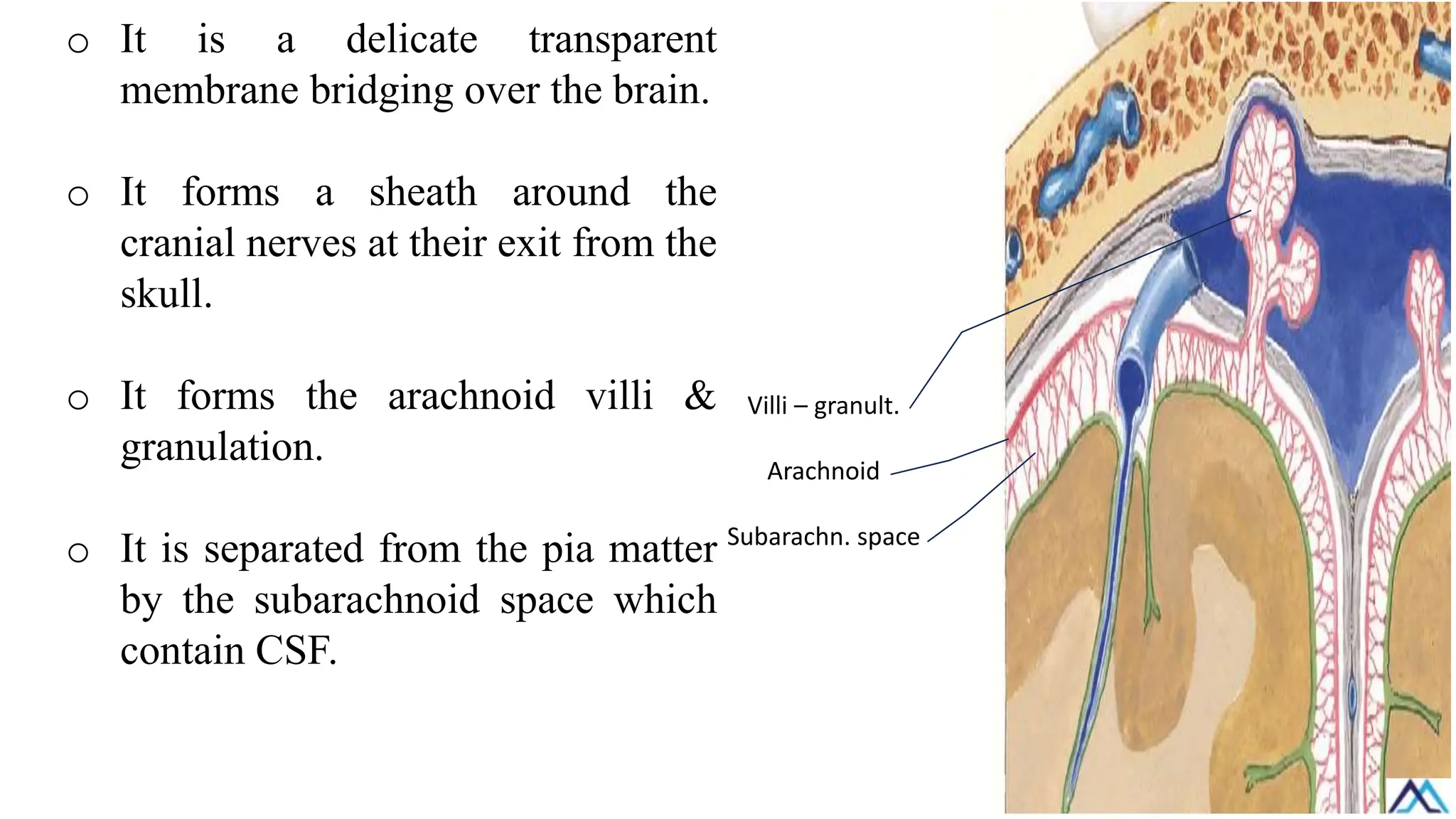
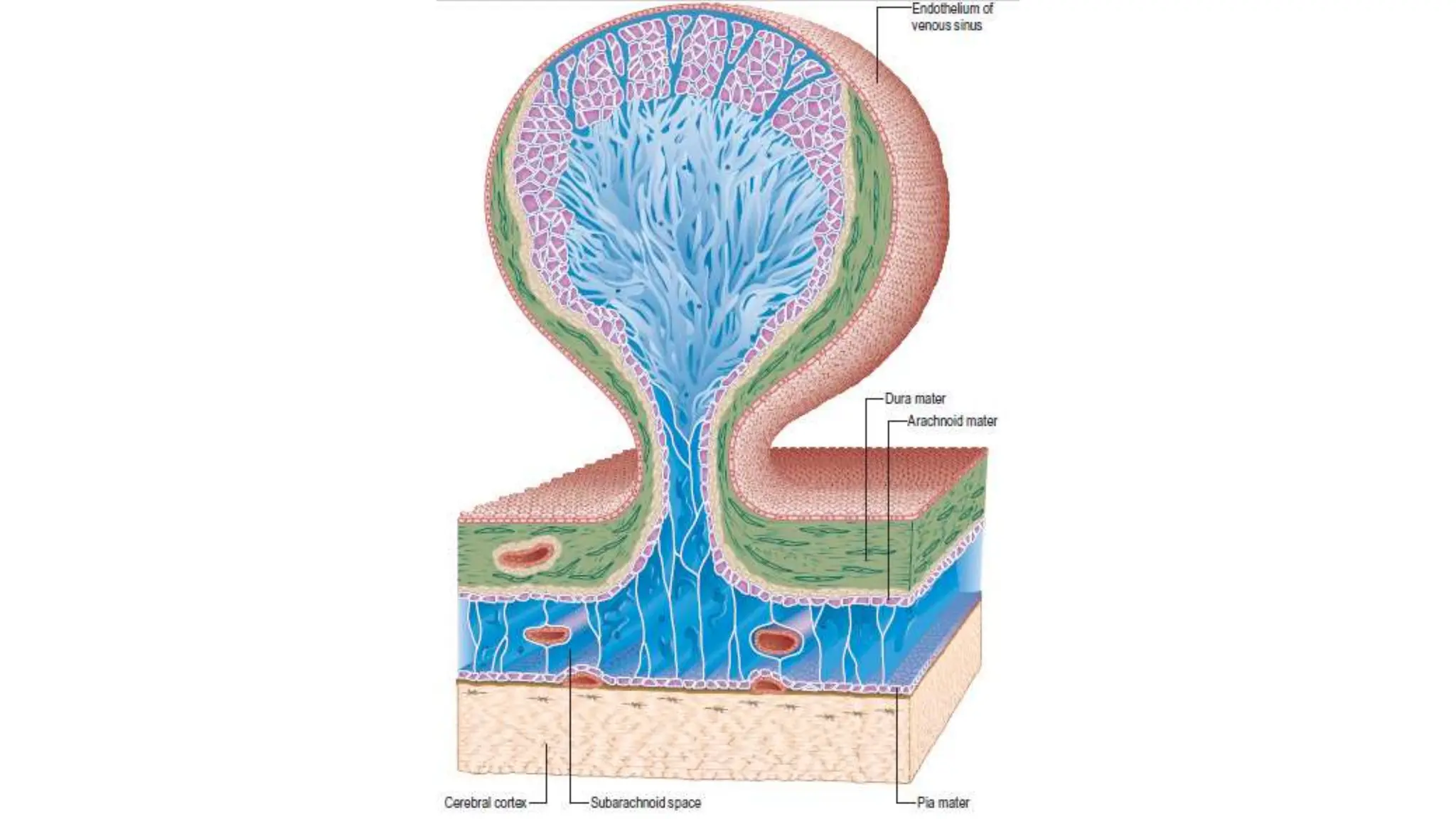
o It isa delicate transparent
membrane bridging over the brain.
o It forms a sheath around the
cranial nerves at their exit from the
skull.
o It forms the arachnoid villi &
granulation.
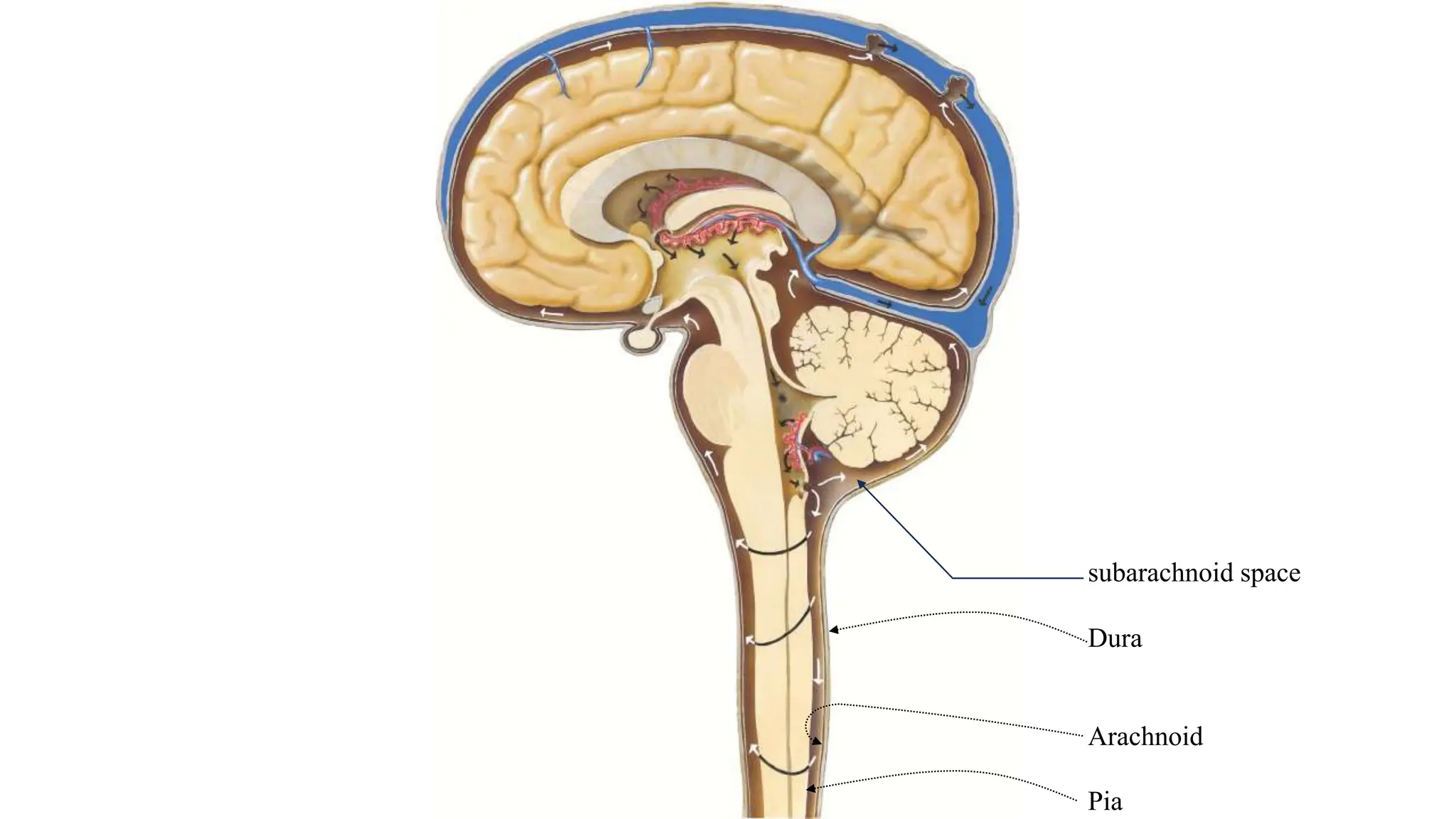
o It is separated from the pia matter
by the subarachnoid space which
contain CSF.
Villi – granult.
Arachnoid
Subarachn. space
56.
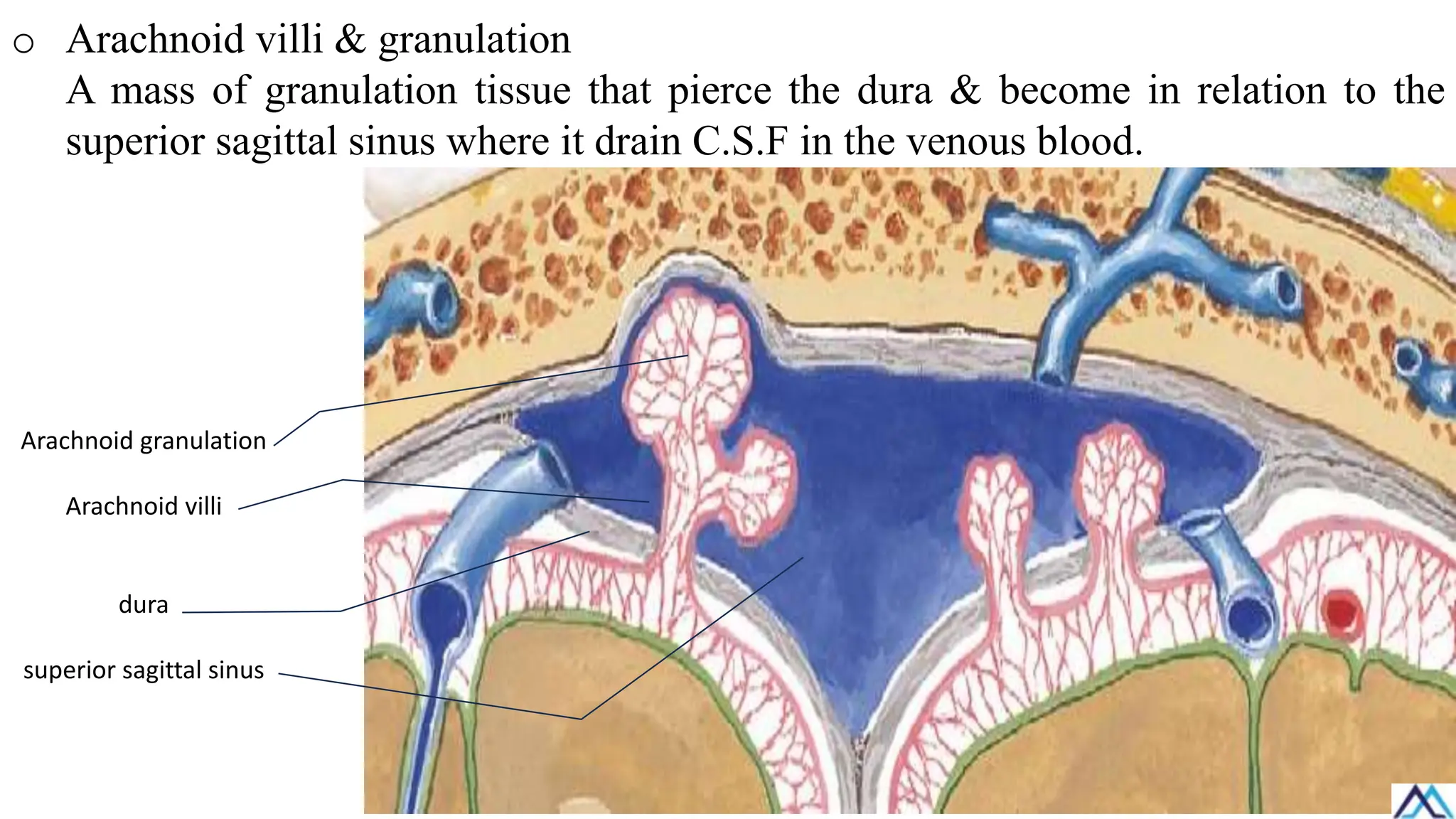
o Arachnoid villi& granulation
A mass of granulation tissue that pierce the dura & become in relation to the
superior sagittal sinus where it drain C.S.F in the venous blood.
Arachnoid granulation
Arachnoid villi
dura
superior sagittal sinus
57.
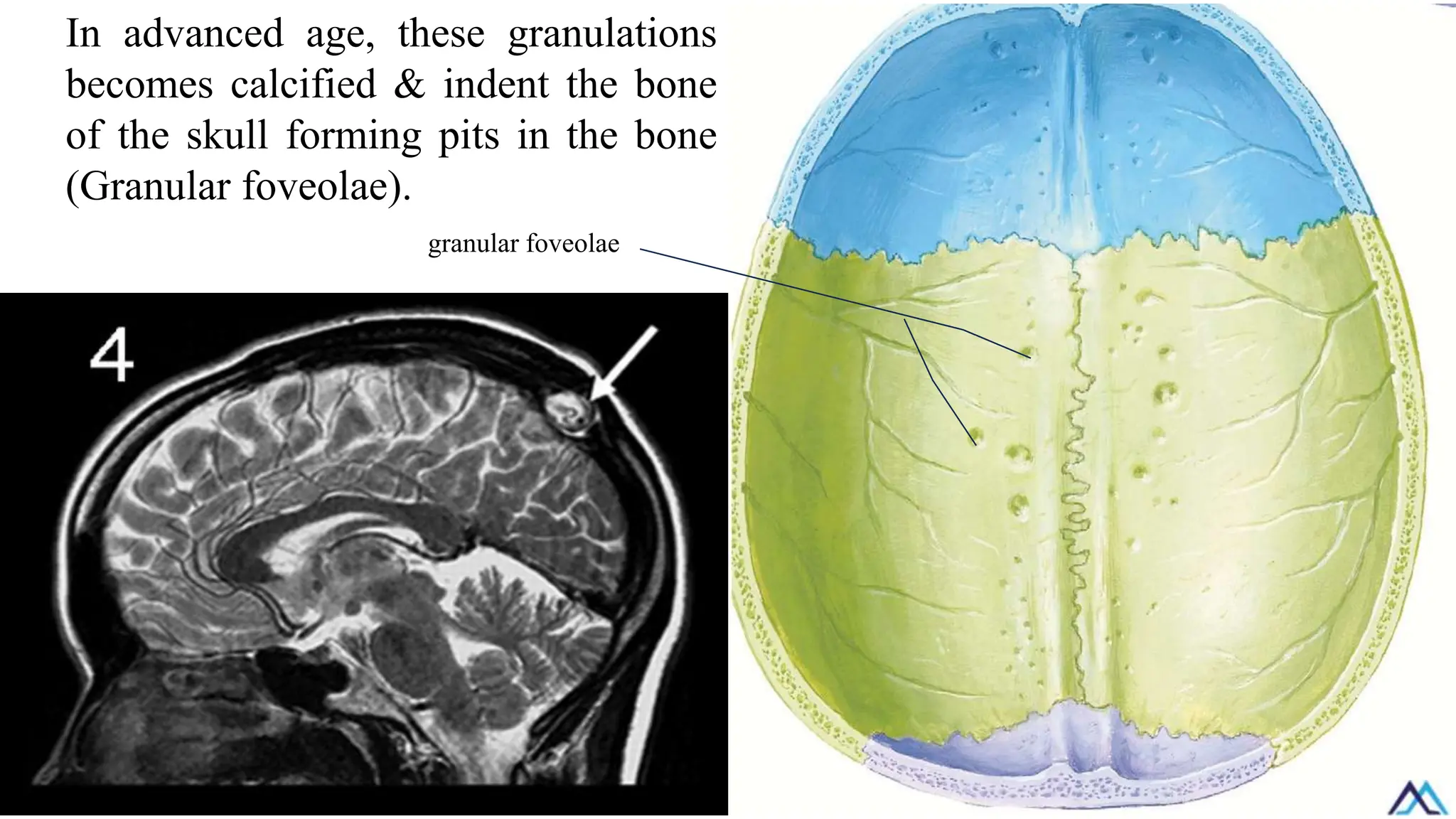
In advanced age,these granulations
becomes calcified & indent the bone
of the skull forming pits in the bone
(Granular foveolae).
granular foveolae
58.
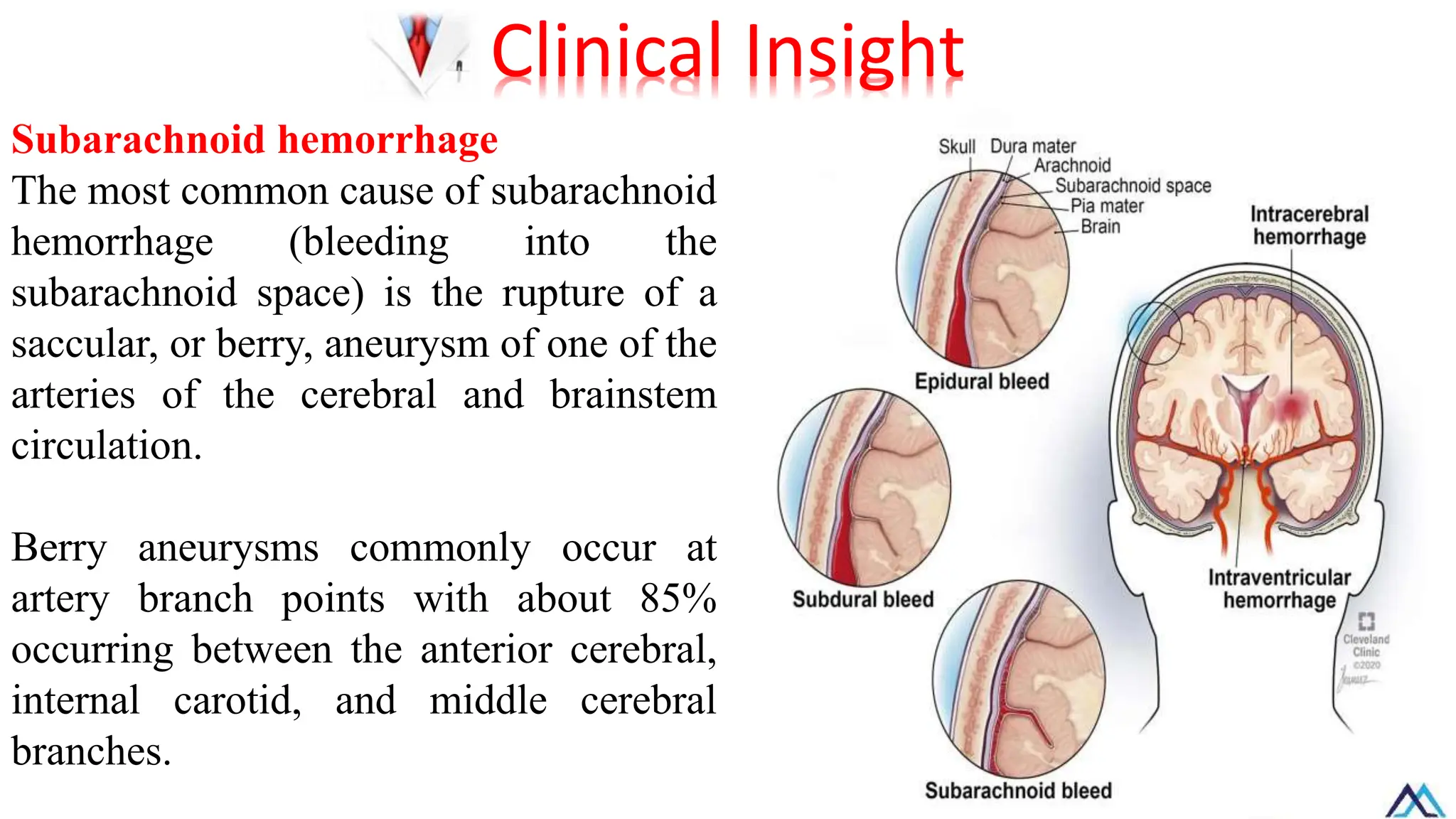
Subarachnoid hemorrhage
The mostcommon cause of subarachnoid
hemorrhage (bleeding into the
subarachnoid space) is the rupture of a
saccular, or berry, aneurysm of one of the
arteries of the cerebral and brainstem
circulation.
Berry aneurysms commonly occur at
artery branch points with about 85%
occurring between the anterior cerebral,
internal carotid, and middle cerebral
branches.
Clinical Insight
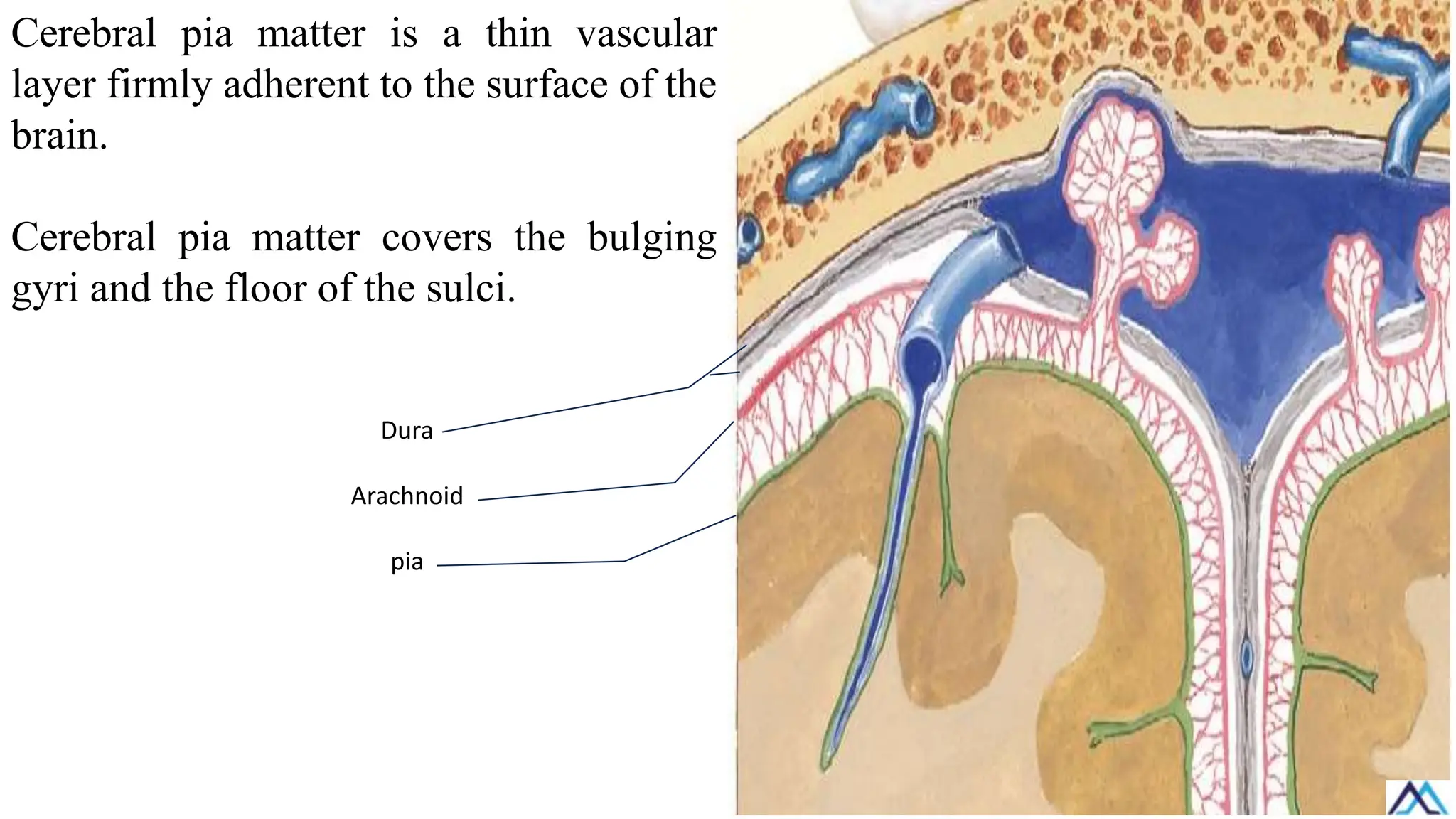
Cerebral pia matteris a thin vascular
layer firmly adherent to the surface of the
brain.
Cerebral pia matter covers the bulging
gyri and the floor of the sulci.
Dura
Arachnoid
pia
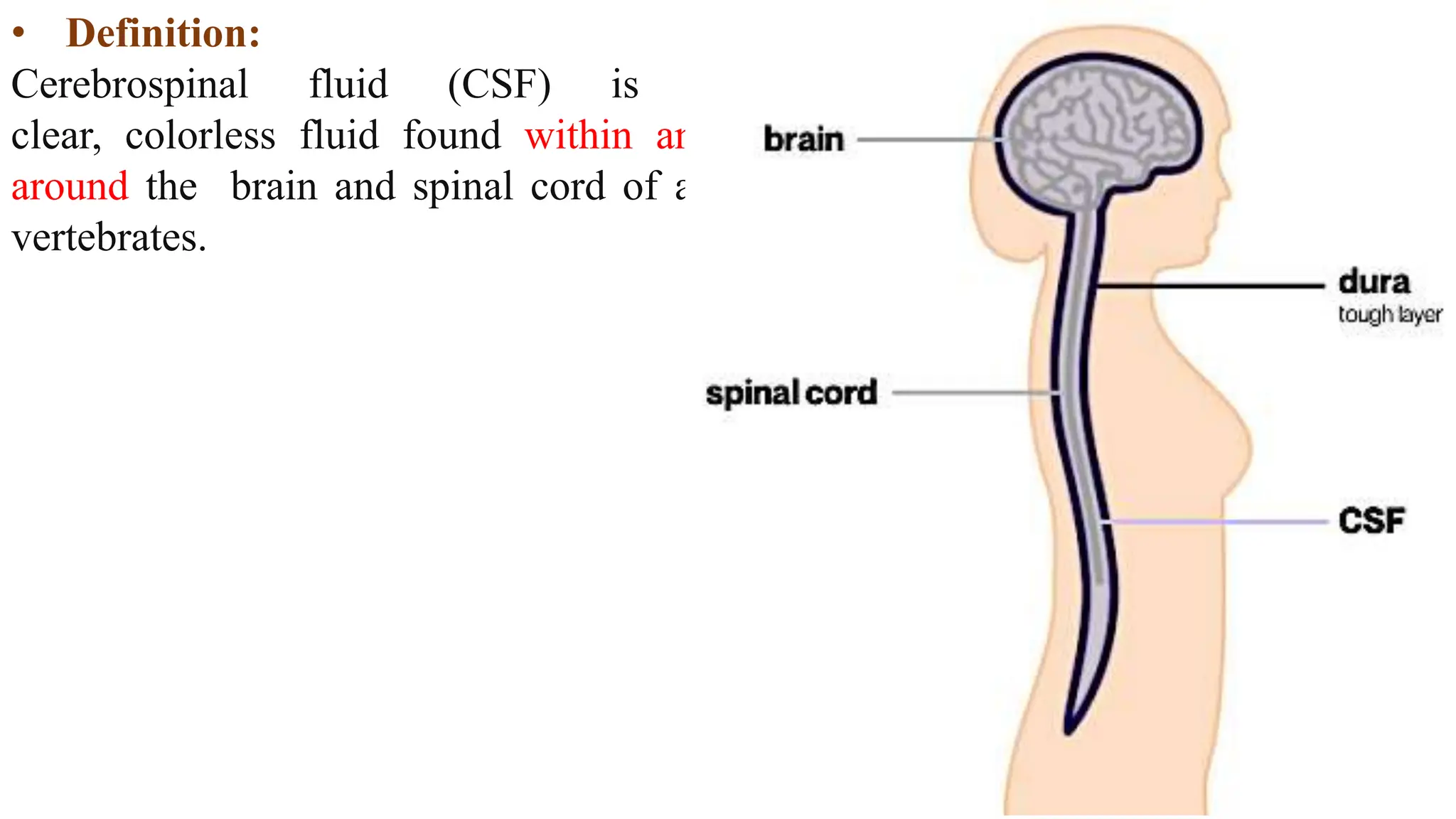
• Definition:
Cerebrospinal fluid(CSF) is a
clear, colorless fluid found within and
around the brain and spinal cord of all
vertebrates.
65.
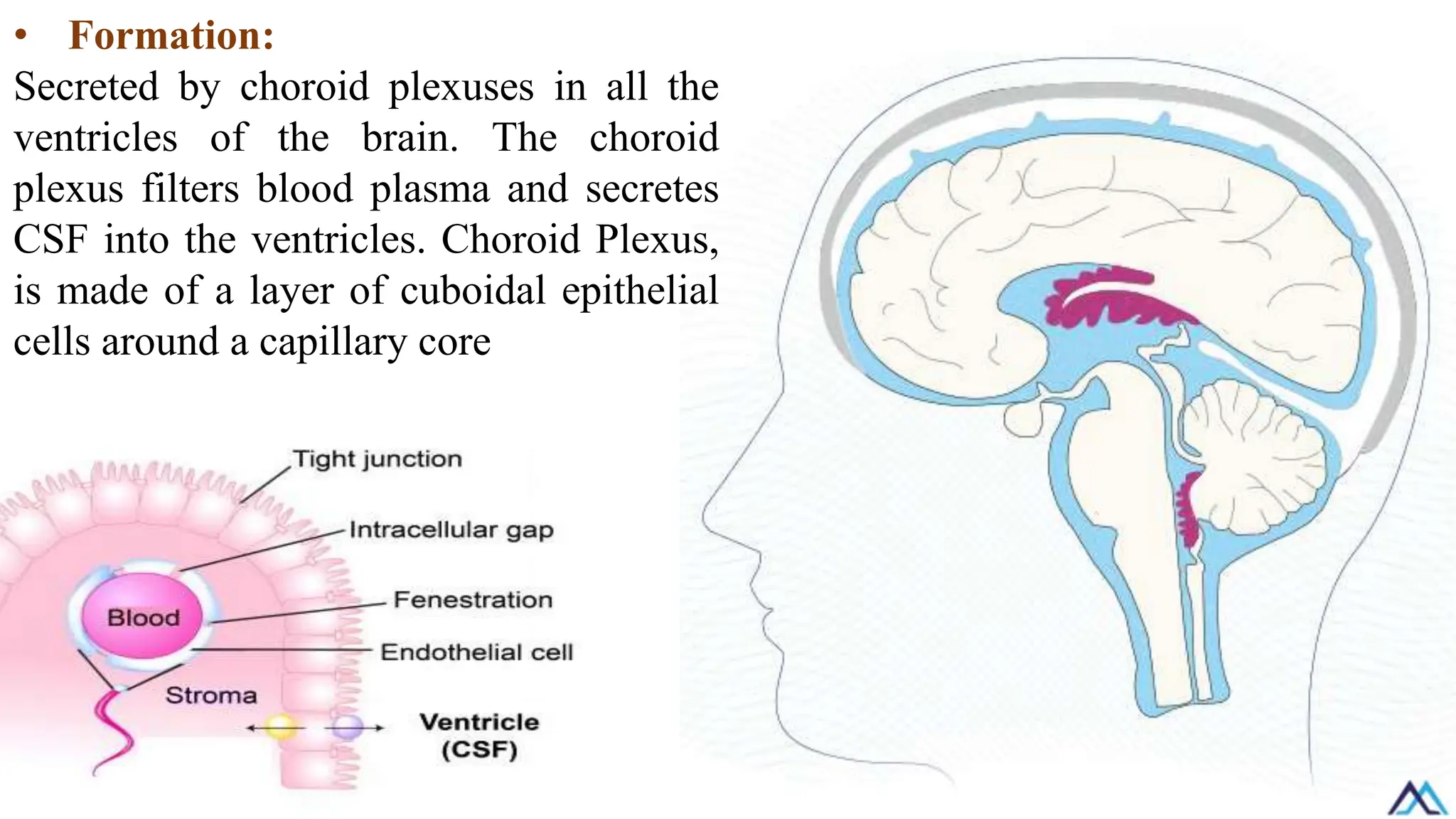
• Formation:
Secreted bychoroid plexuses in all the
ventricles of the brain. The choroid
plexus filters blood plasma and secretes
CSF into the ventricles. Choroid Plexus,
is made of a layer of cuboidal epithelial
cells around a capillary core
66.
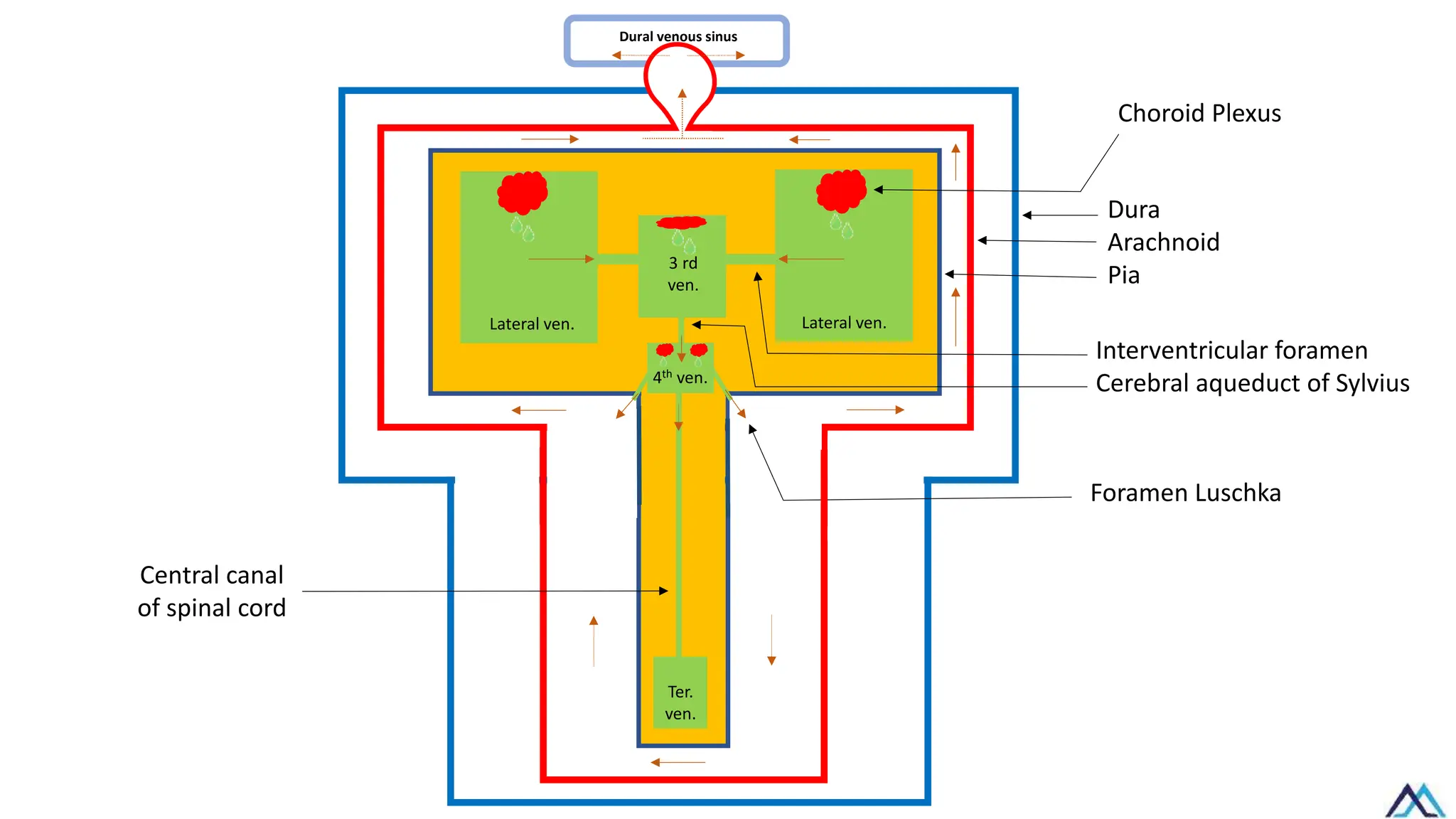
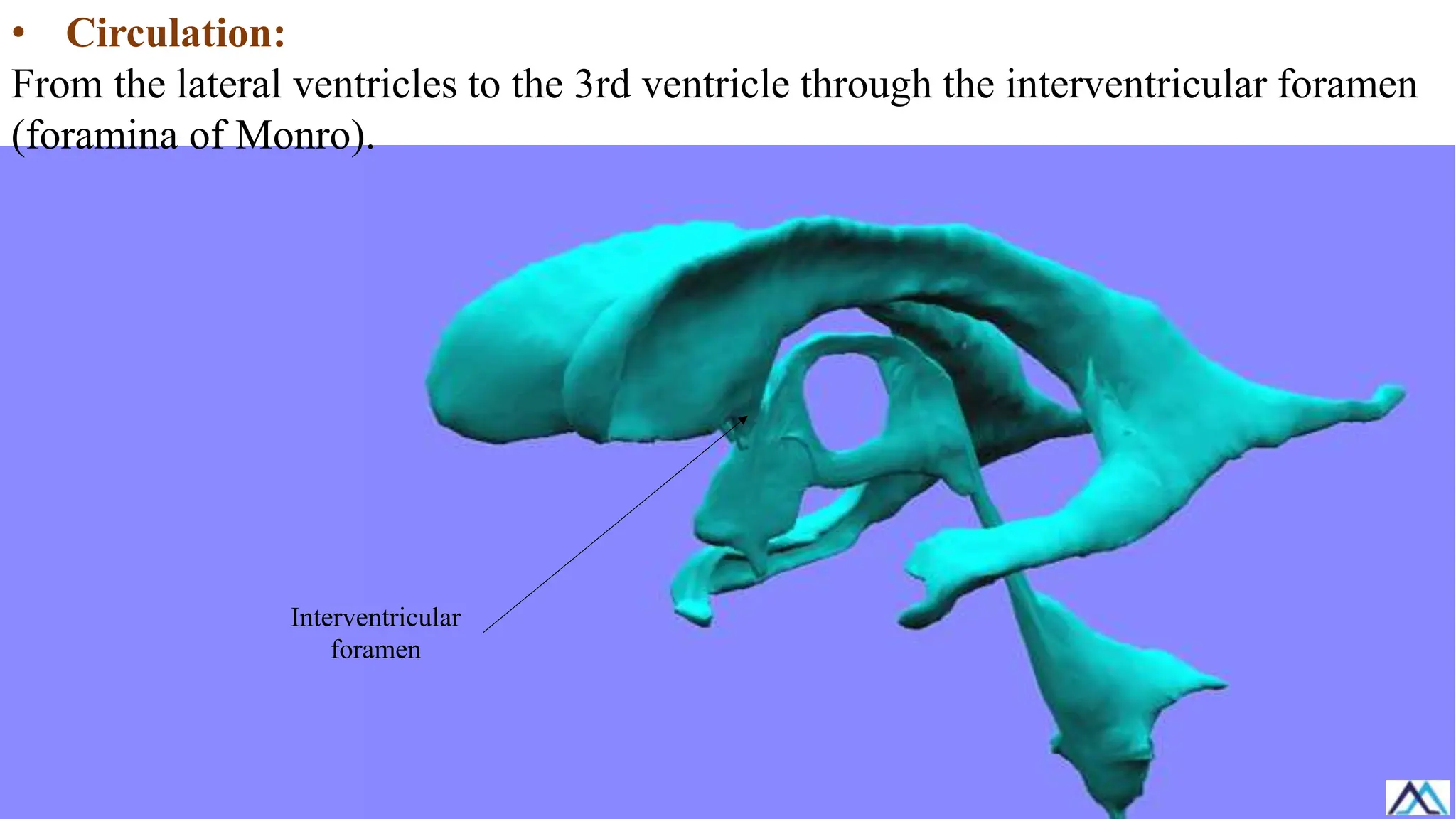
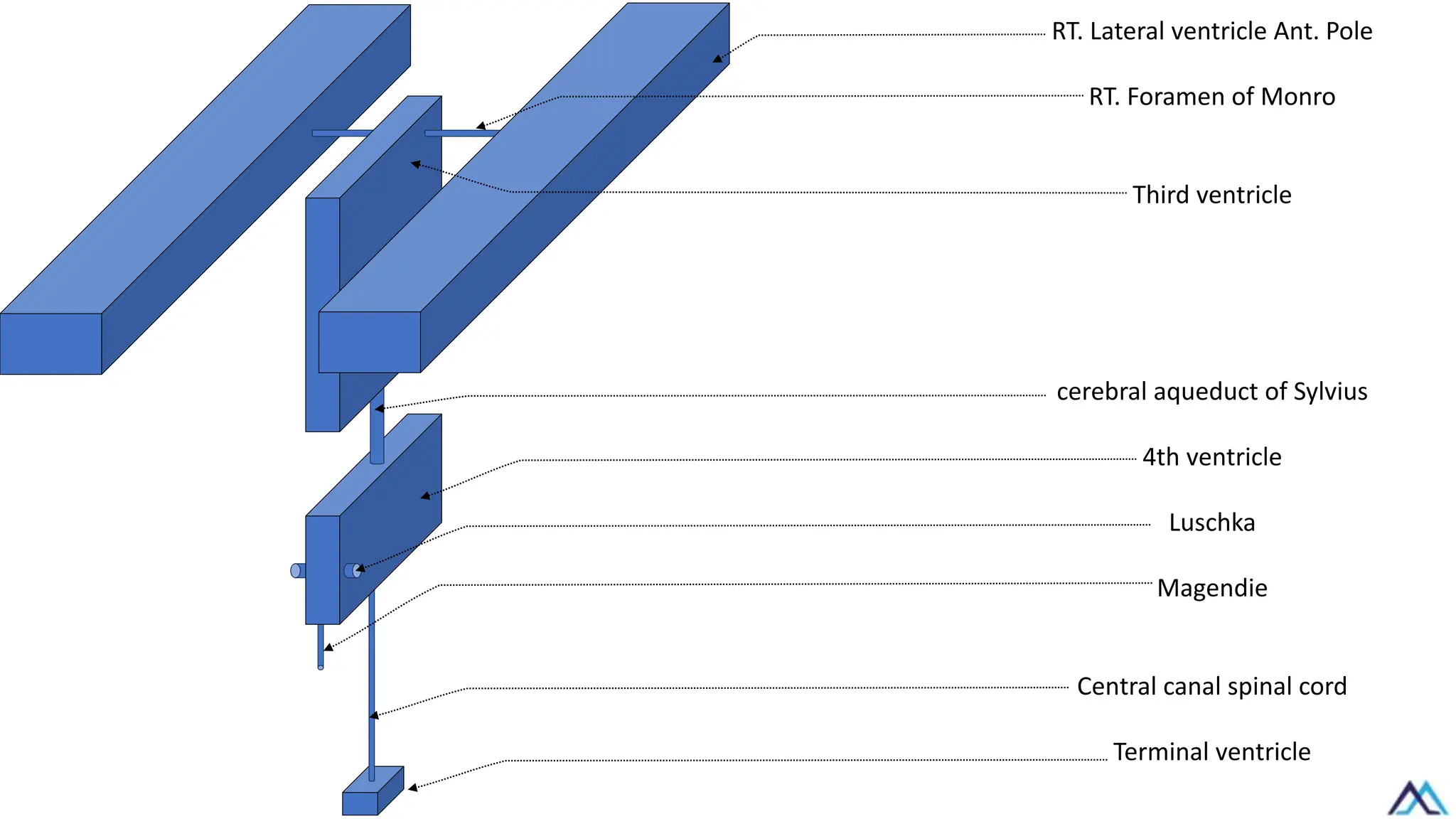
• Circulation:
From thelateral ventricles to the 3rd ventricle through the interventricular foramen
(foramina of Monro).
Interventricular
foramen
67.
RT. Lateral ventricleAnt. Pole
RT. Foramen of Monro
Third ventricle
cerebral aqueduct of Sylvius
4th ventricle
Luschka
Magendie
Central canal spinal cord
Terminal ventricle
68.
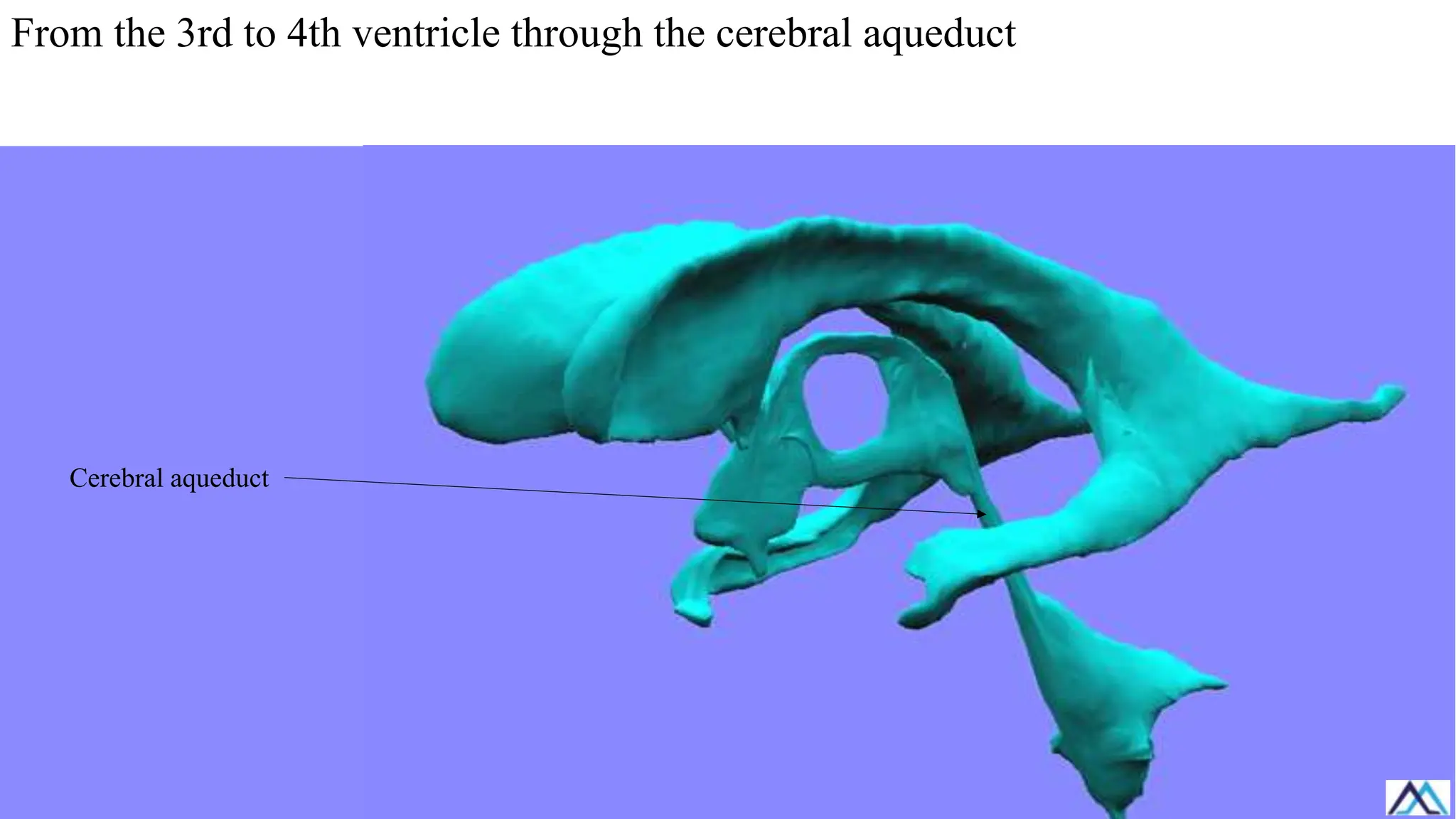
From the 3rdto 4th ventricle through the cerebral aqueduct
Cerebral aqueduct
69.
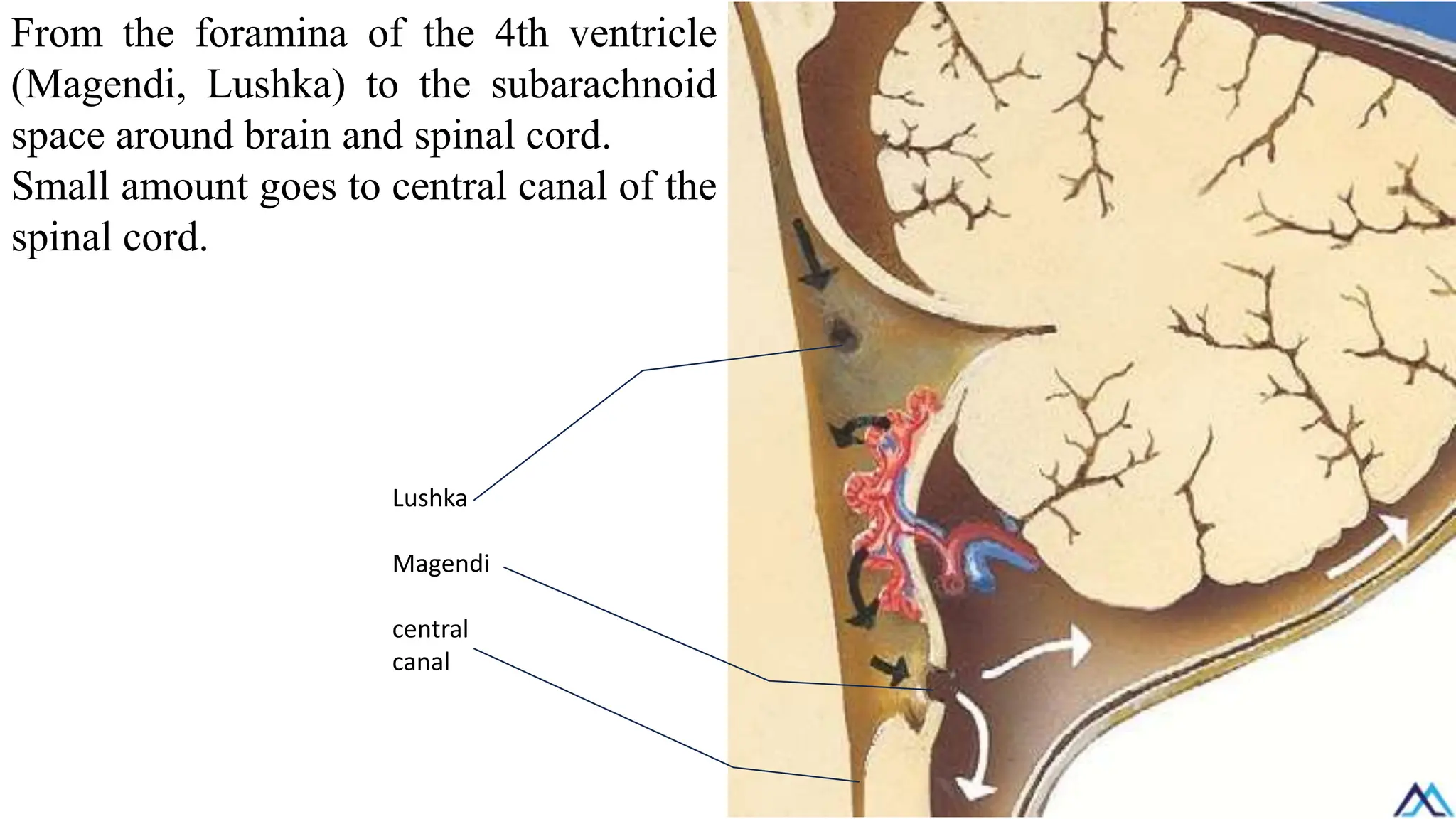
From the foraminaof the 4th ventricle
(Magendi, Lushka) to the subarachnoid
space around brain and spinal cord.
Small amount goes to central canal of the
spinal cord.
Lushka
Magendi
central
canal
70.
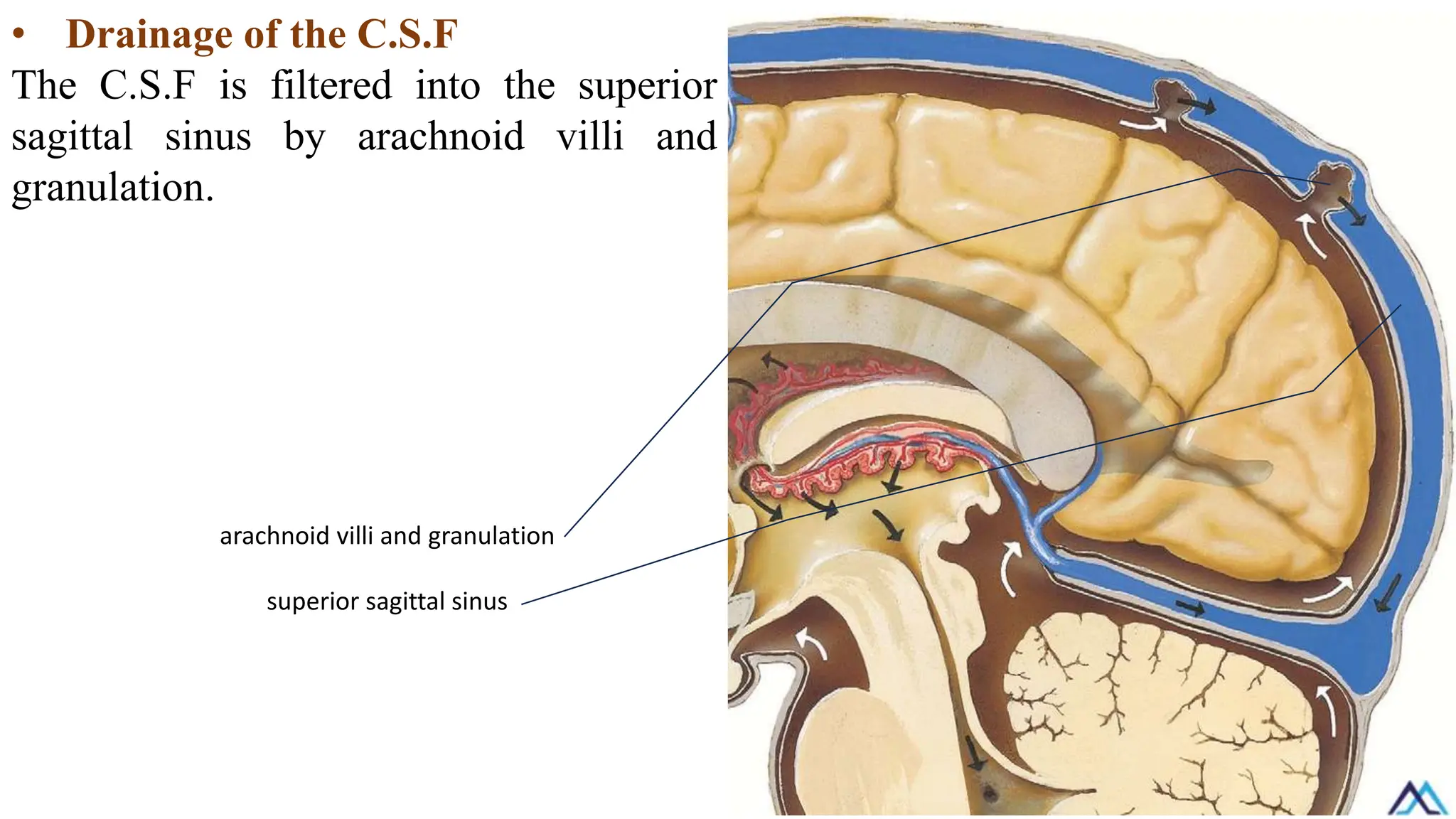
• Drainage ofthe C.S.F
The C.S.F is filtered into the superior
sagittal sinus by arachnoid villi and
granulation.
arachnoid villi and granulation
superior sagittal sinus
72.
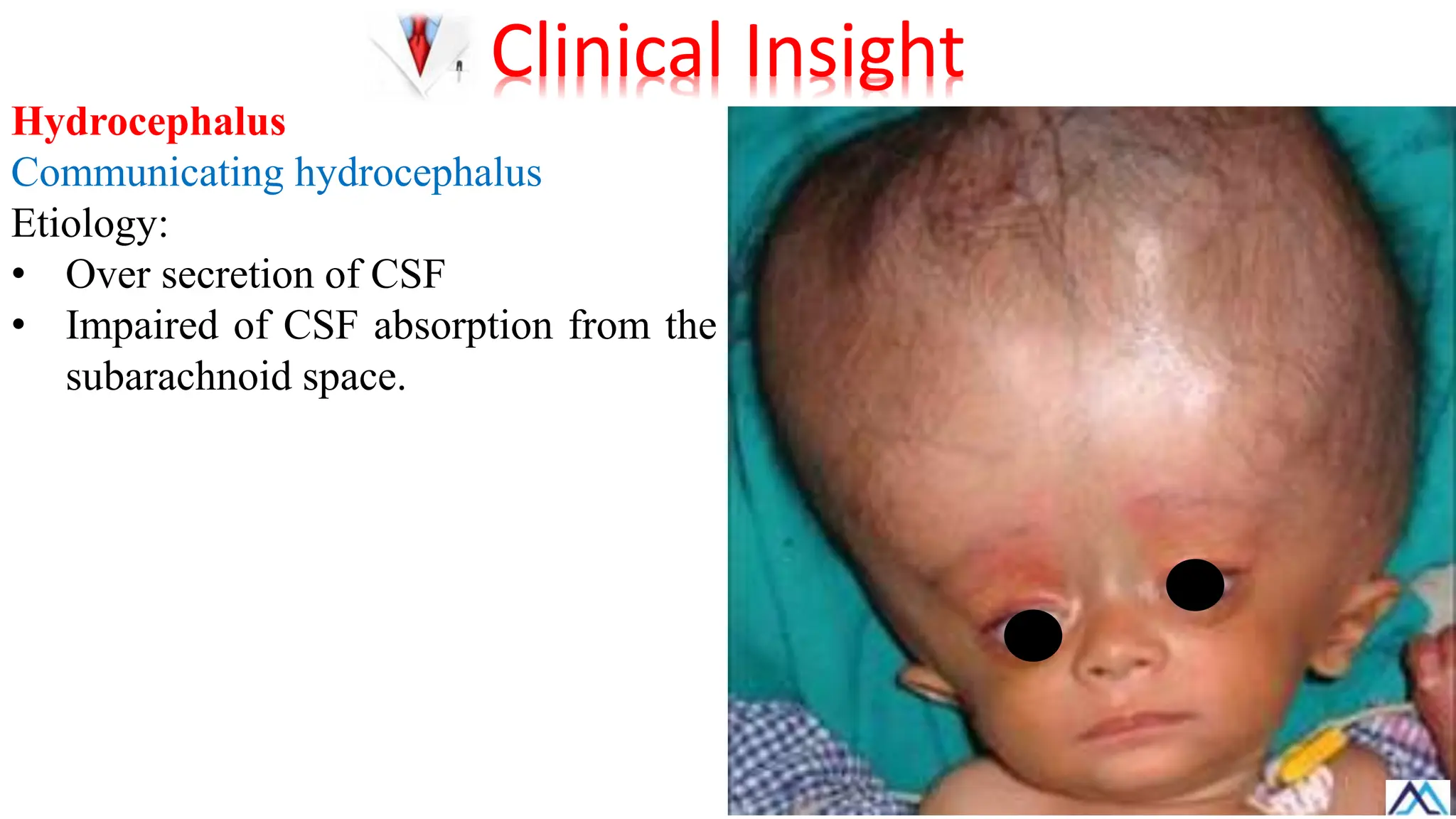
Hydrocephalus
Obstruction of thedrainage system leads
to distension of the ventricles, a case
called hydrocephalus.
Clinical Insight
73.
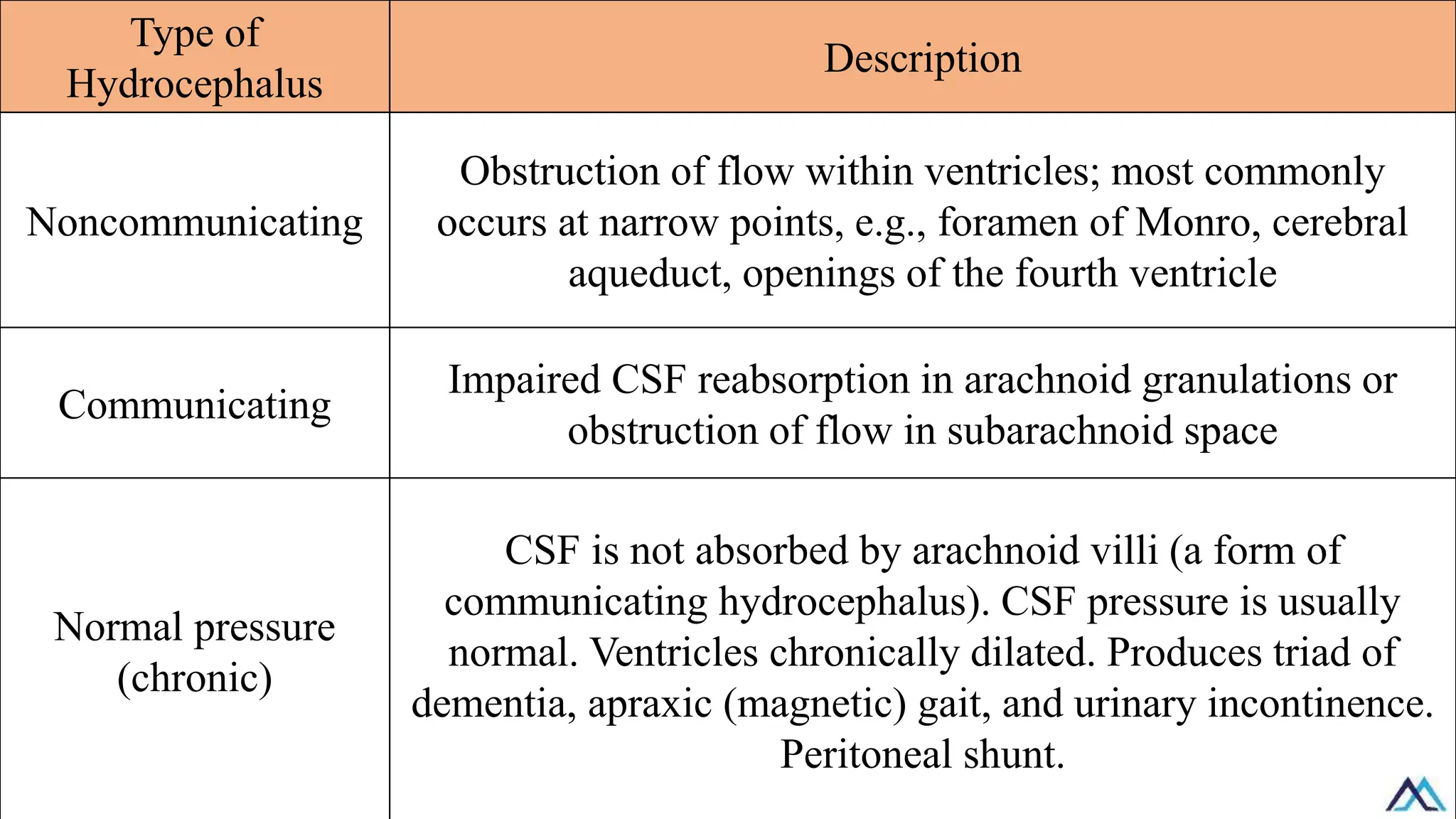
Type of
Hydrocephalus
Description
Noncommunicating
Obstruction offlow within ventricles; most commonly
occurs at narrow points, e.g., foramen of Monro, cerebral
aqueduct, openings of the fourth ventricle
Communicating
Impaired CSF reabsorption in arachnoid granulations or
obstruction of flow in subarachnoid space
Normal pressure
(chronic)
CSF is not absorbed by arachnoid villi (a form of
communicating hydrocephalus). CSF pressure is usually
normal. Ventricles chronically dilated. Produces triad of
dementia, apraxic (magnetic) gait, and urinary incontinence.
Peritoneal shunt.
74.
Hydrocephalus
This condition occurswhen excess
cerebrospinal fluid (CSF) collects in the
brain’s ventricles.
Obstructive (noncommunicating)
hydrocephalus
Etiology:
• Blockage at any point in the
ventricular system
• Stenosis of the cerebral aqueduct (of
Sylvius)
Clinical Insight
Normal pressure hydrocephalus
NPHis a type of communicating hydrocephalus caused by impaired cerebrospinal
fluid absorption.
It manifests with a classic triad of symptoms:
• Urinary incontinence
• Gait disturbance
• Cognitive decline.
Clinical Insight
77.
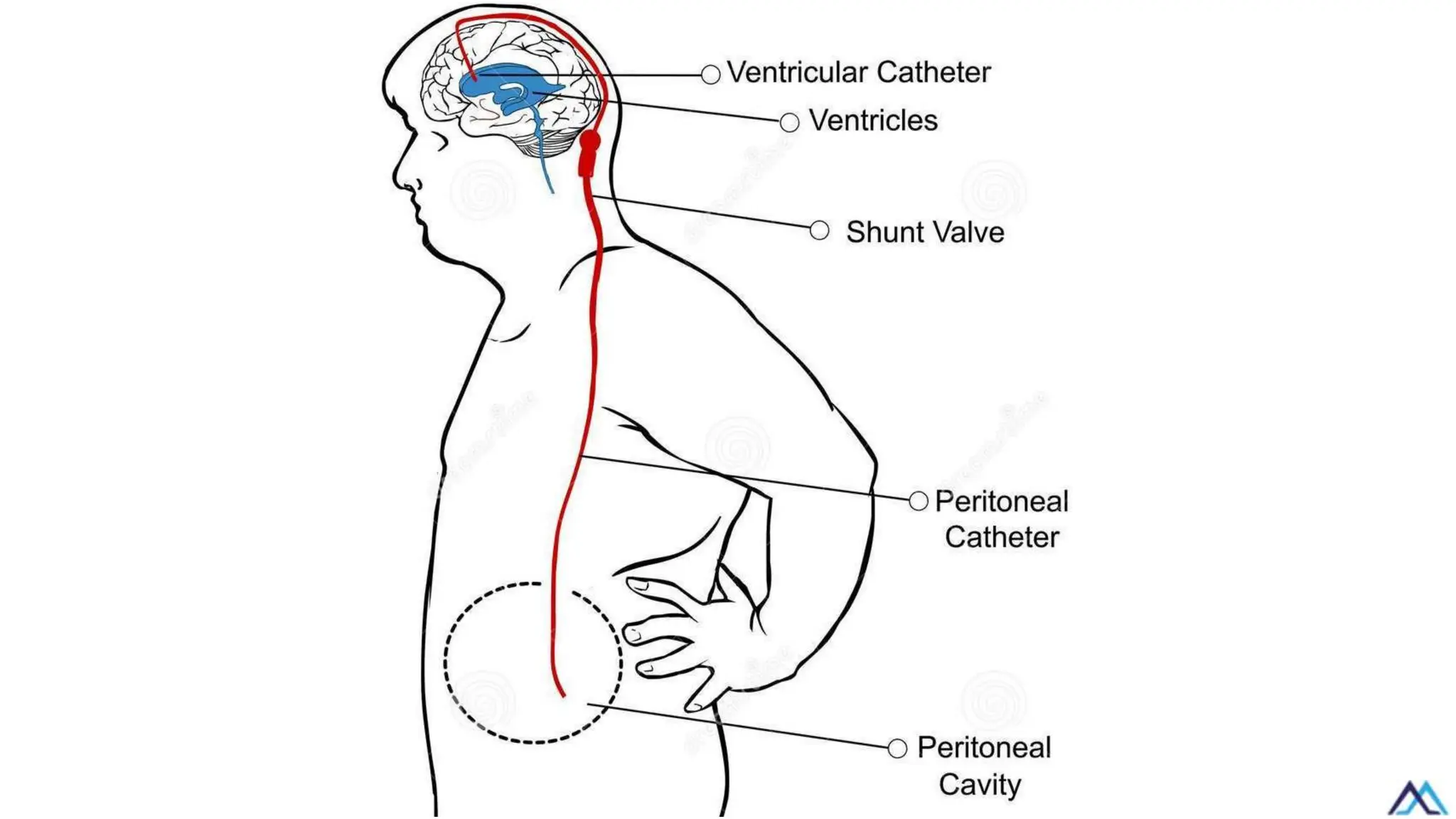
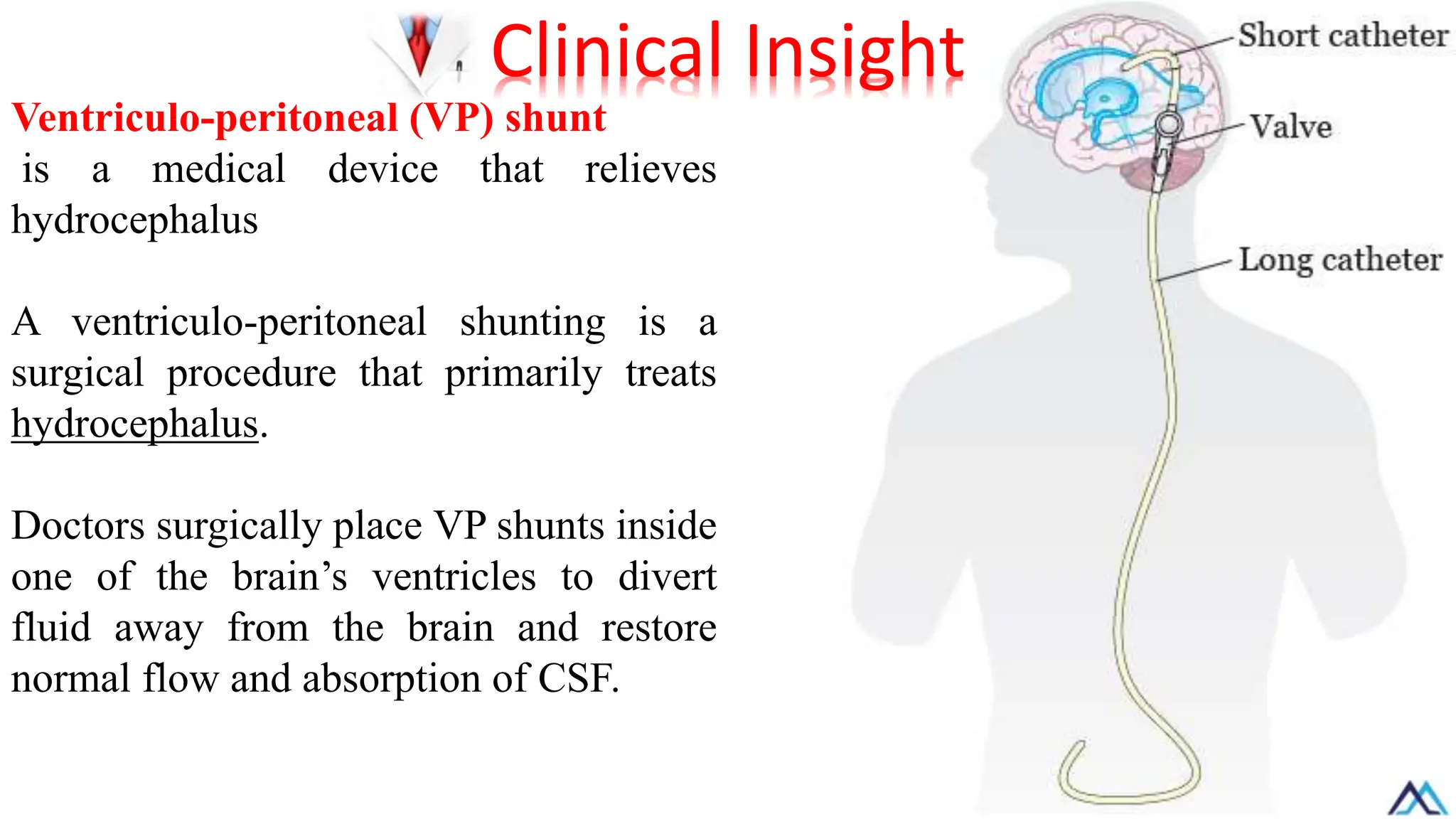
Ventriculo-peritoneal (VP) shunt
isa medical device that relieves
hydrocephalus
A ventriculo-peritoneal shunting is a
surgical procedure that primarily treats
hydrocephalus.
Doctors surgically place VP shunts inside
one of the brain’s ventricles to divert
fluid away from the brain and restore
normal flow and absorption of CSF.
Clinical Insight
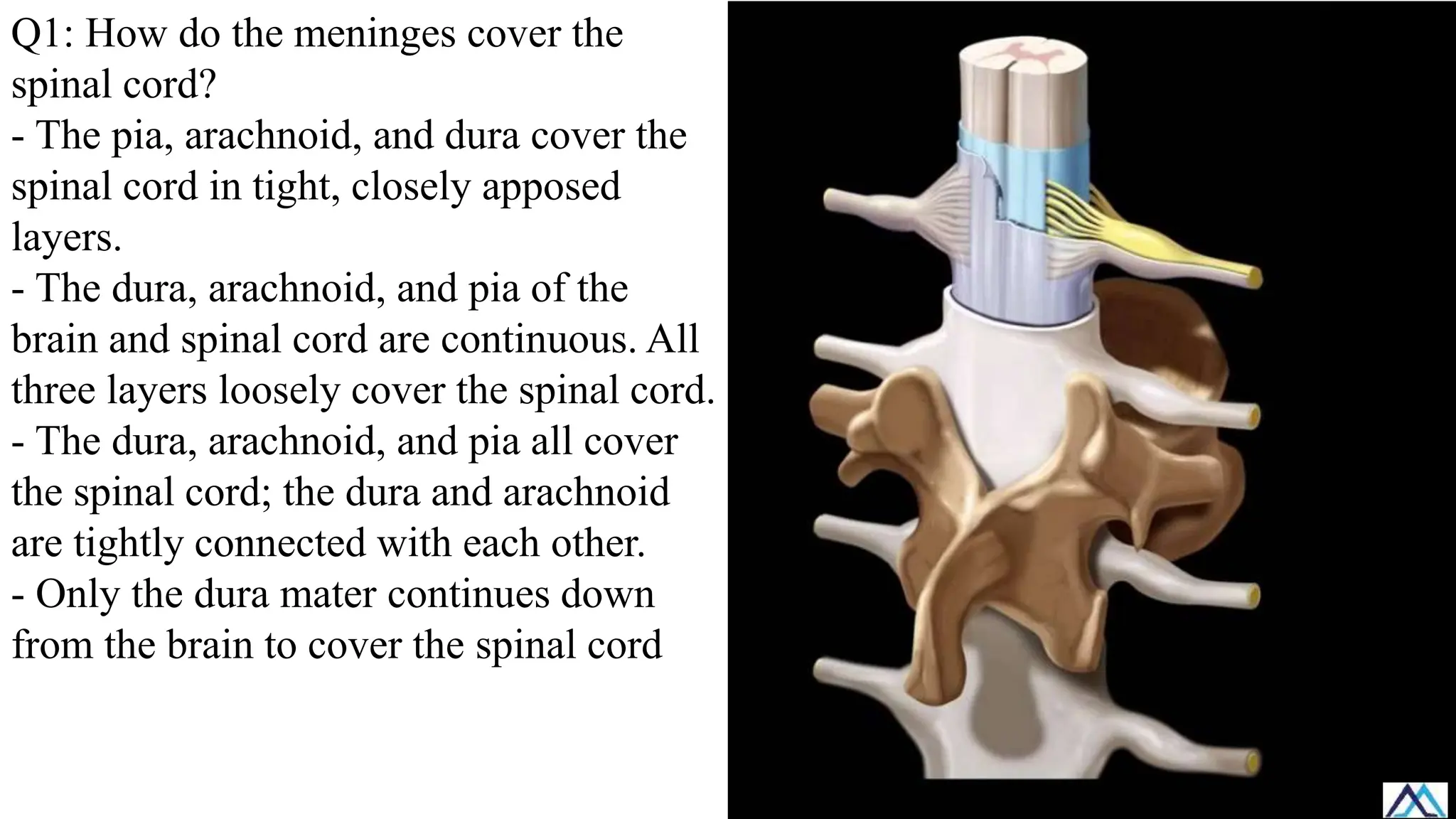
Q1: How dothe meninges cover the
spinal cord?
- The pia, arachnoid, and dura cover the
spinal cord in tight, closely apposed
layers.
- The dura, arachnoid, and pia of the
brain and spinal cord are continuous. All
three layers loosely cover the spinal cord.
- The dura, arachnoid, and pia all cover
the spinal cord; the dura and arachnoid
are tightly connected with each other.
- Only the dura mater continues down
from the brain to cover the spinal cord
80.
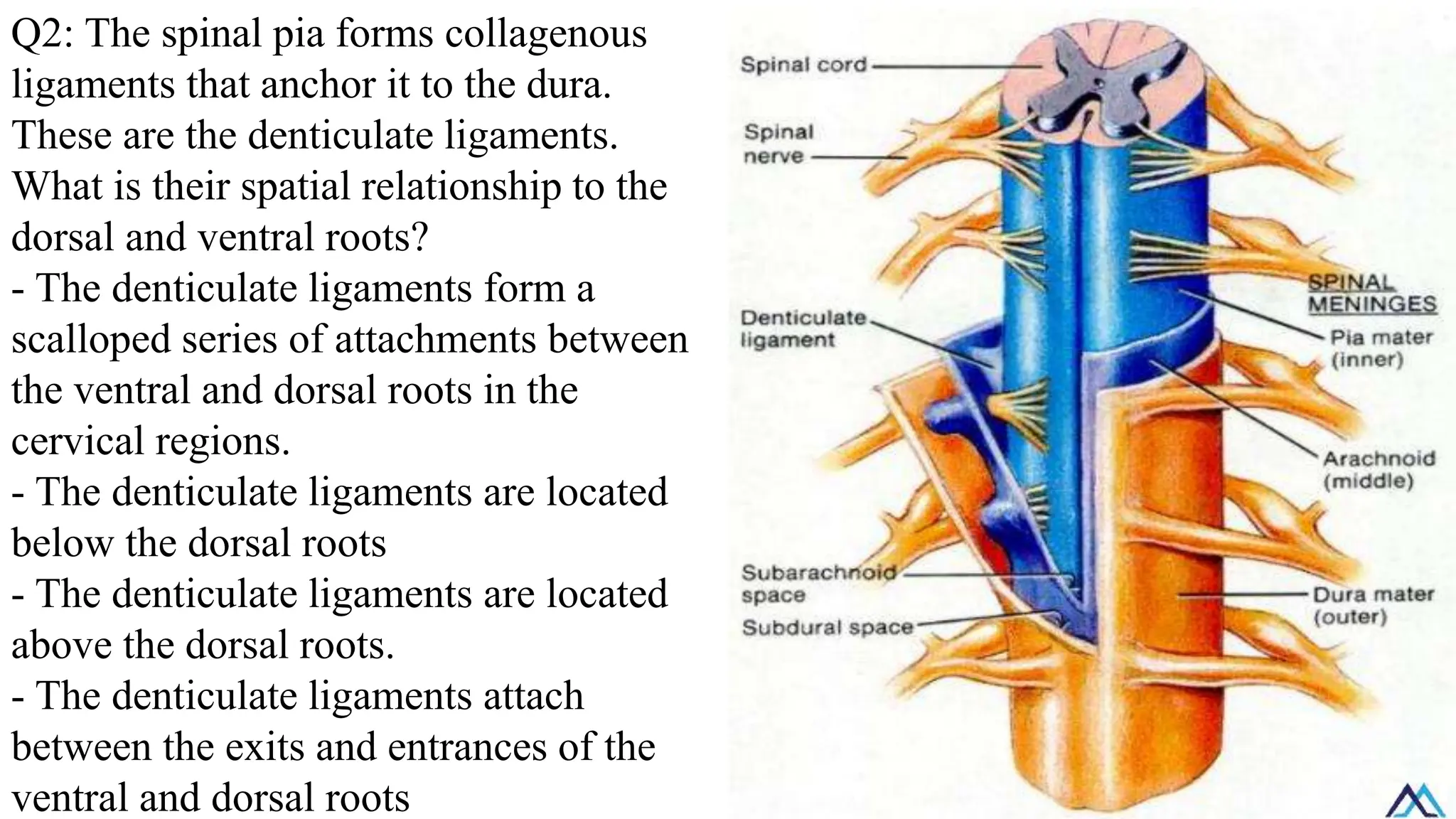
Q2: The spinalpia forms collagenous
ligaments that anchor it to the dura.
These are the denticulate ligaments.
What is their spatial relationship to the
dorsal and ventral roots?
- The denticulate ligaments form a
scalloped series of attachments between
the ventral and dorsal roots in the
cervical regions.
- The denticulate ligaments are located
below the dorsal roots
- The denticulate ligaments are located
above the dorsal roots.
- The denticulate ligaments attach
between the exits and entrances of the
ventral and dorsal roots
81.
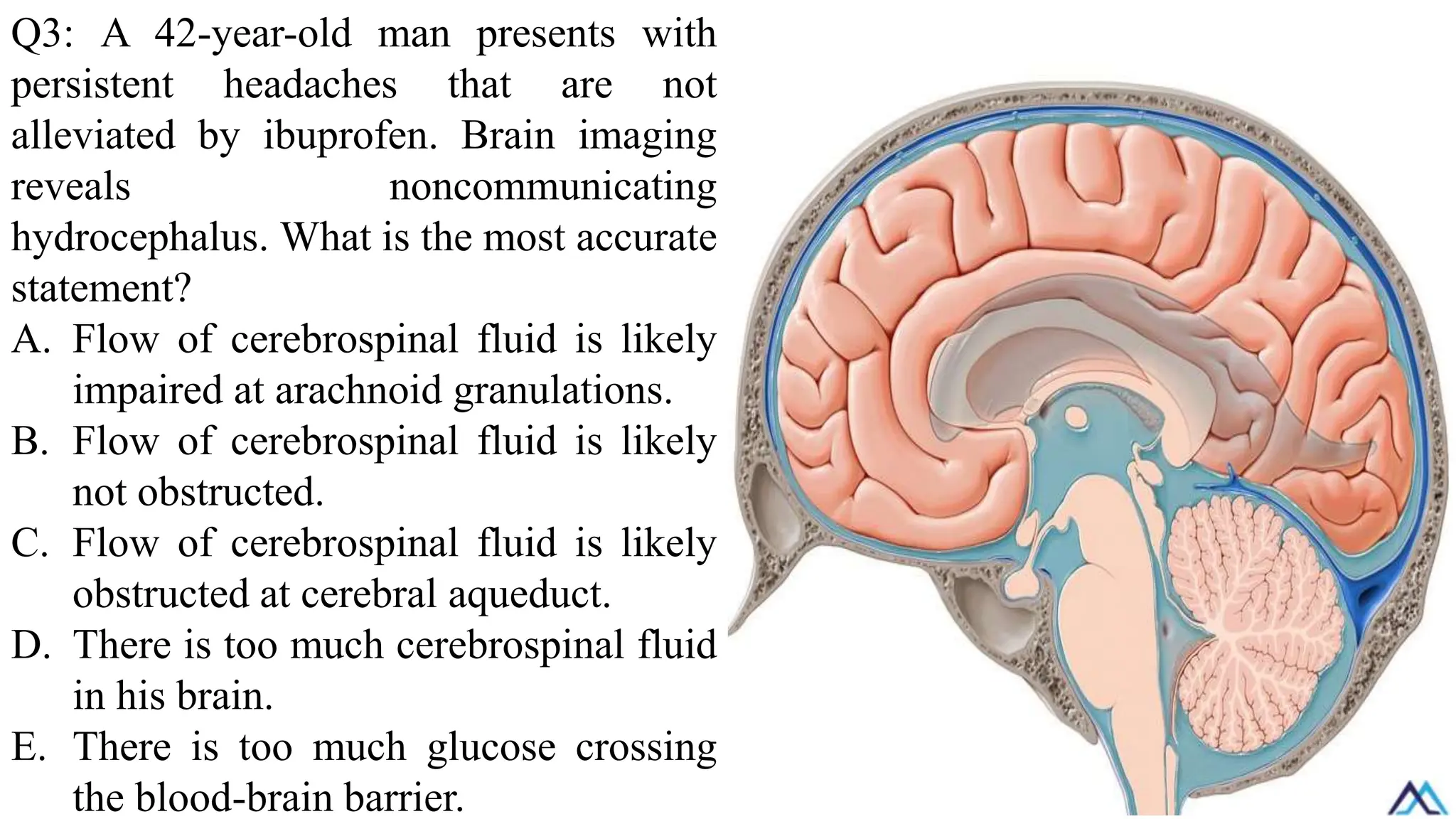
Q3: A 42-year-oldman presents with
persistent headaches that are not
alleviated by ibuprofen. Brain imaging
reveals noncommunicating
hydrocephalus. What is the most accurate
statement?
A. Flow of cerebrospinal fluid is likely
impaired at arachnoid granulations.
B. Flow of cerebrospinal fluid is likely
not obstructed.
C. Flow of cerebrospinal fluid is likely
obstructed at cerebral aqueduct.
D. There is too much cerebrospinal fluid
in his brain.
E. There is too much glucose crossing
the blood-brain barrier.
82.
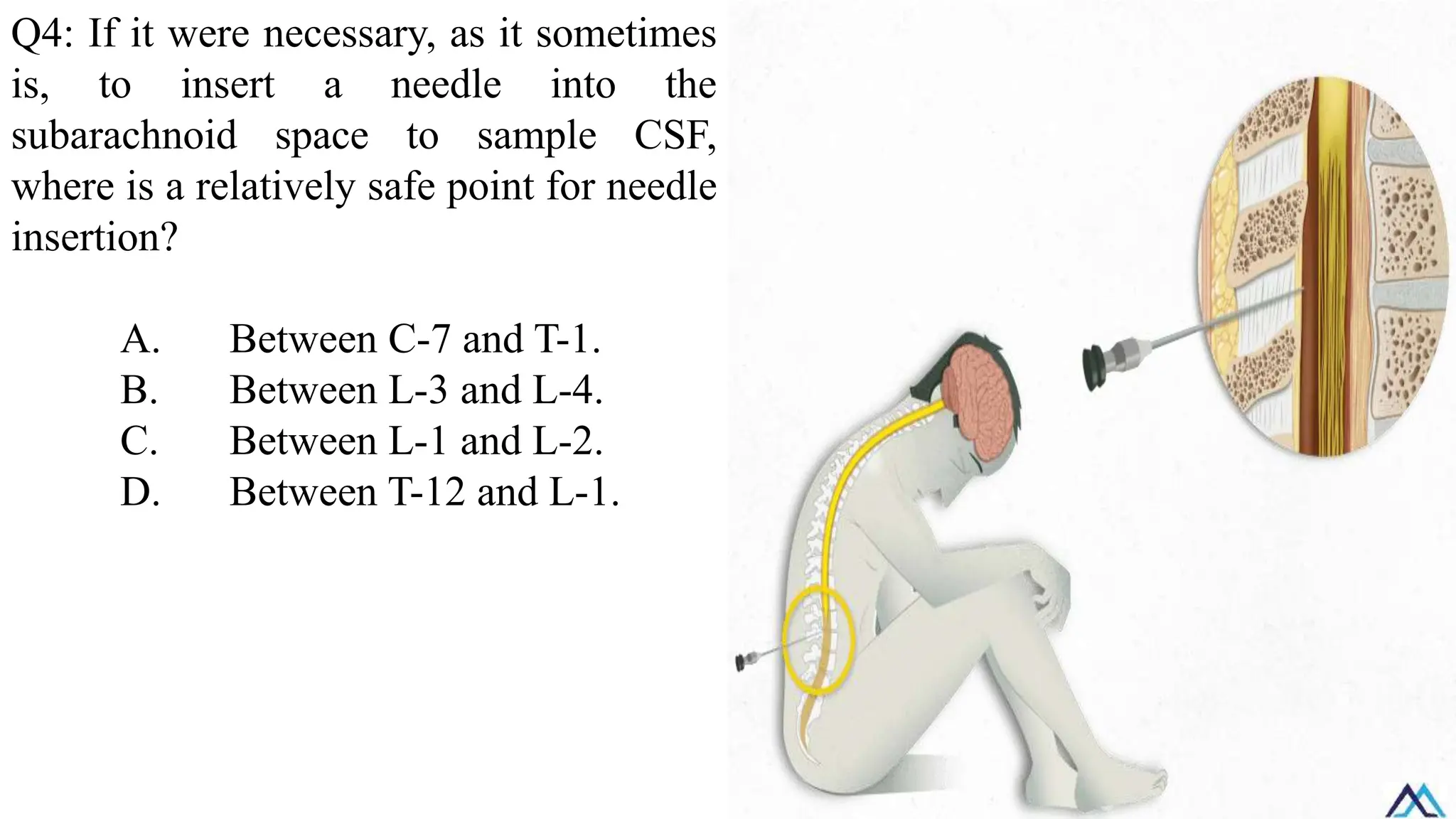
Q4: If itwere necessary, as it sometimes
is, to insert a needle into the
subarachnoid space to sample CSF,
where is a relatively safe point for needle
insertion?
A. Between C-7 and T-1.
B. Between L-3 and L-4.
C. Between L-1 and L-2.
D. Between T-12 and L-1.
83.
Q5: A 78-year-oldman comes to the
physician for evaluation after a fall. His
history is significant for worsening
urinary incontinence and memory loss
over the past 4 months with wide-based
gait with short steps and bradykinesia
without tremor. Funduscopic
examination is normal. Serum thyroid-
stimulating hormone is 2.2 mIU/L.
Which of the following conditions is the
most likely cause of this patient’s recent
decline?
Alzheimer disease
Hypothyroidism
Multi-infarct dementia
Normal pressure hydrocephalus
84.
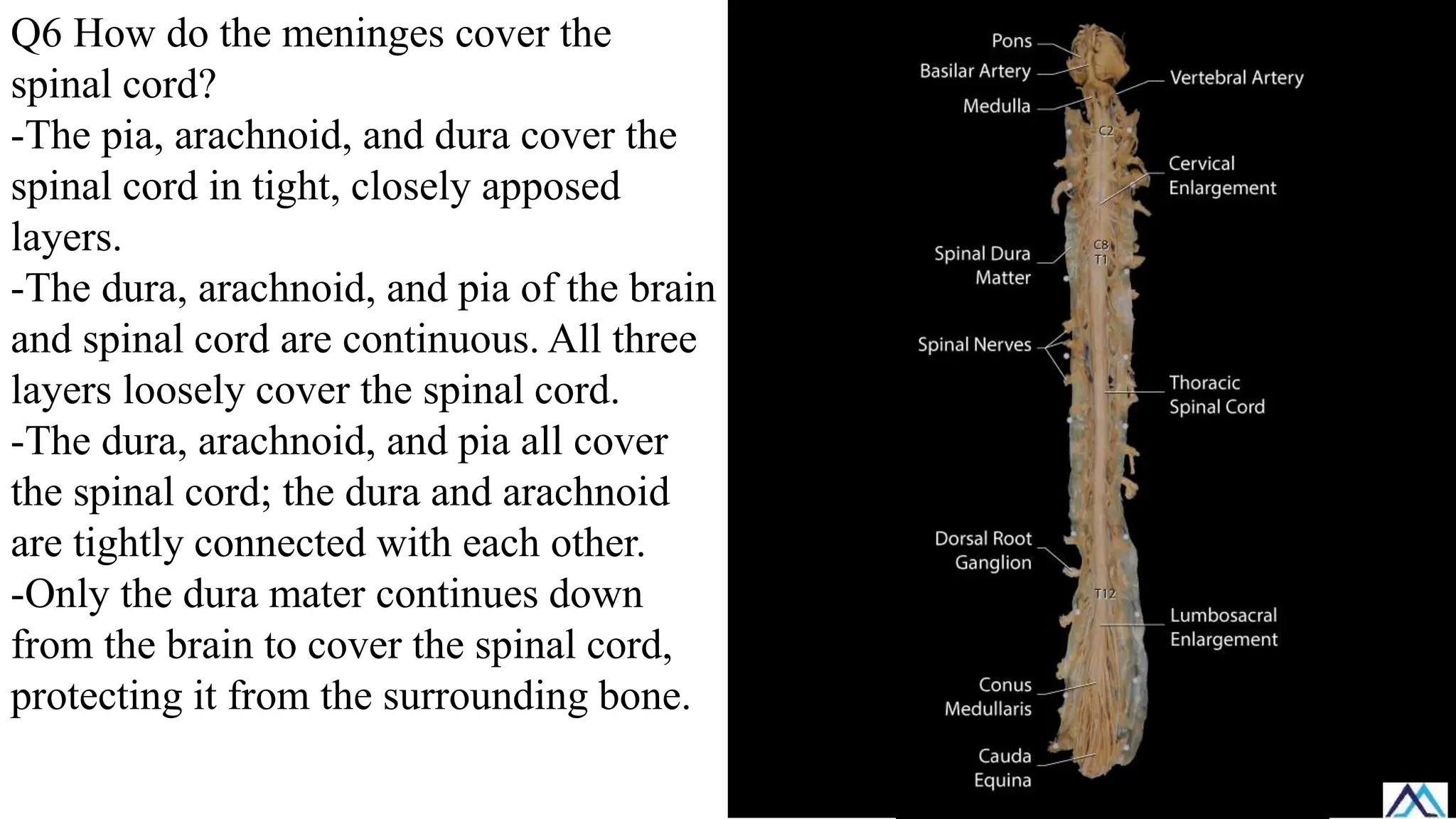
Q6 How dothe meninges cover the
spinal cord?
-The pia, arachnoid, and dura cover the
spinal cord in tight, closely apposed
layers.
-The dura, arachnoid, and pia of the brain
and spinal cord are continuous. All three
layers loosely cover the spinal cord.
-The dura, arachnoid, and pia all cover
the spinal cord; the dura and arachnoid
are tightly connected with each other.
-Only the dura mater continues down
from the brain to cover the spinal cord,
protecting it from the surrounding bone.
85.
Q7 A 4-month-oldinfant is brought to
the hospital with irritability, high fever,
and bulging fontanelle. The pediatrician
suspects meningitis and plans a lumbar
puncture to obtain cerebrospinal fluid for
diagnostic testing. Considering the
anatomical differences in the infant’s
spinal cord termination compared to
adults, the safest site for needle insertion
is:
A. Between L-4 and L-5
B. Between L-3 and L-4
C. Between T-12 and L-1
D. Between C-7 and T-1
86.
Q8 A 22-year-oldman presents with a
severe headache and photophobia. A
lumbar puncture confirms bacterial
meningitis, with purulent CSF. The
infection primarily involves the
leptomeninges, which include two
closely associated layers. Which two
meningeal layers form the
leptomeninges?
A. Dura mater and arachnoid mater
B. Arachnoid mater and pia mater
C. Periosteal dura and meningeal dura
D. Pia mater and dura mater
E. Subarachnoid and subdural spaces
87.
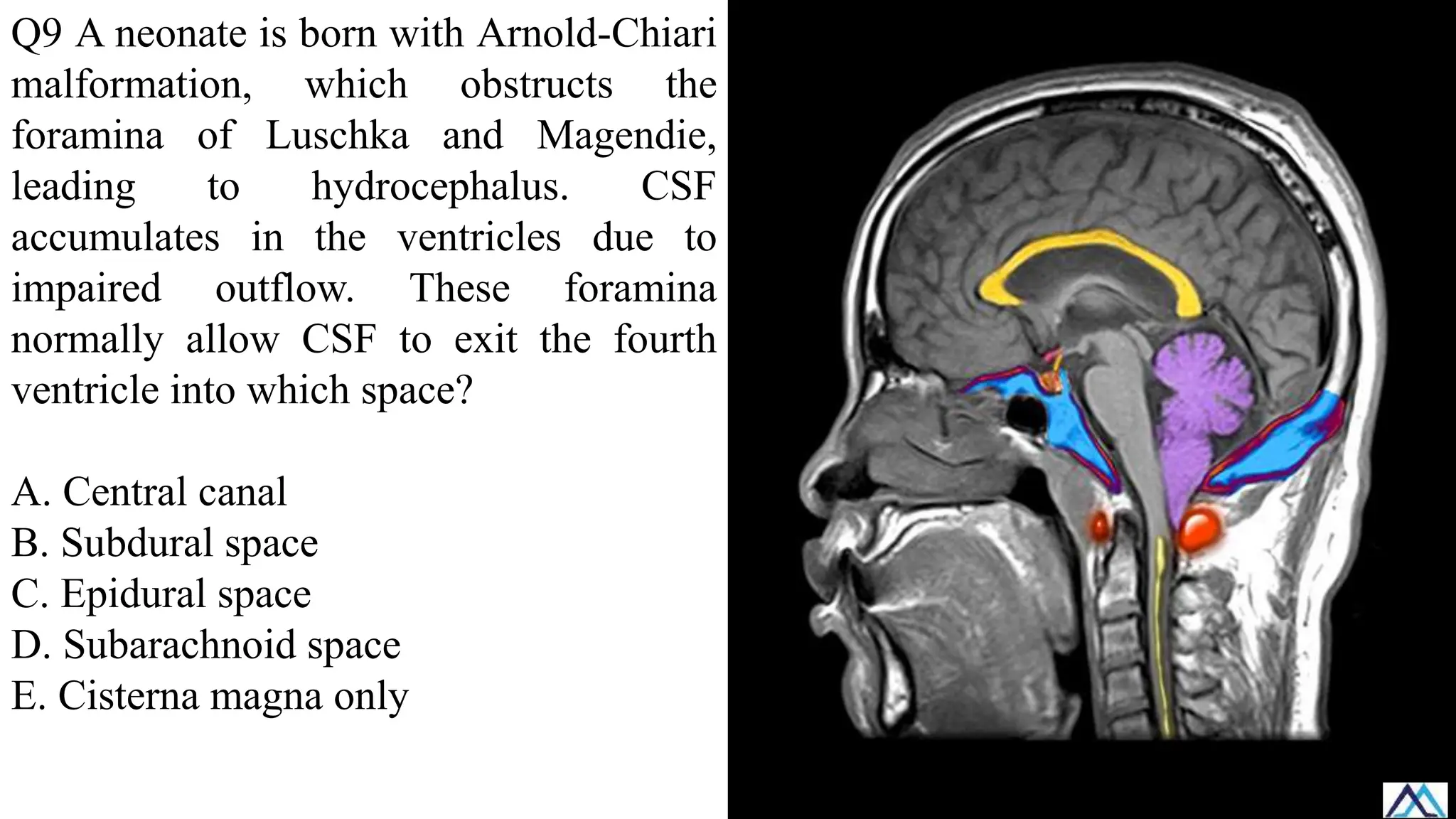
Q9 A neonateis born with Arnold-Chiari
malformation, which obstructs the
foramina of Luschka and Magendie,
leading to hydrocephalus. CSF
accumulates in the ventricles due to
impaired outflow. These foramina
normally allow CSF to exit the fourth
ventricle into which space?
A. Central canal
B. Subdural space
C. Epidural space
D. Subarachnoid space
E. Cisterna magna only
88.
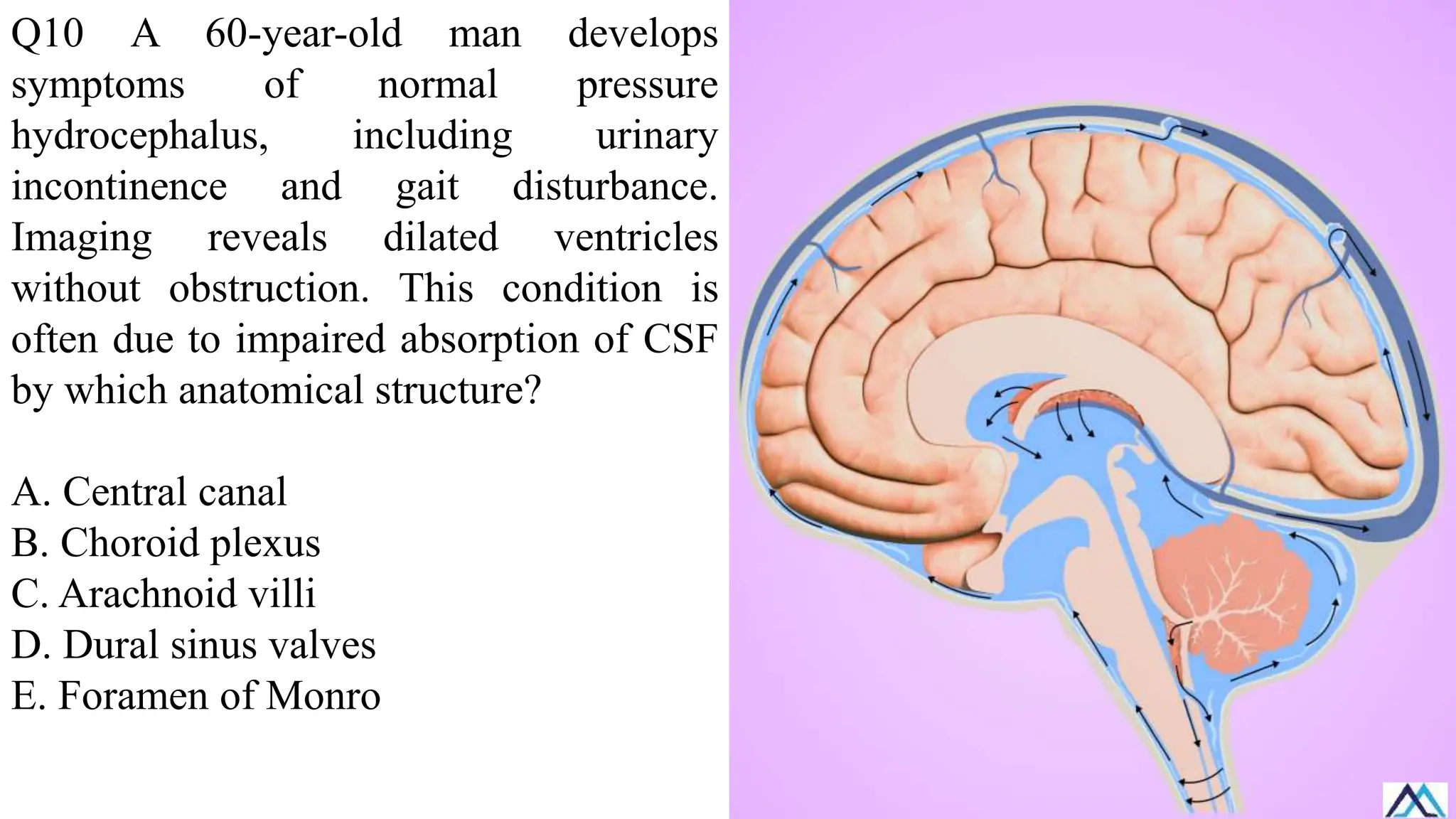
Q10 A 60-year-oldman develops
symptoms of normal pressure
hydrocephalus, including urinary
incontinence and gait disturbance.
Imaging reveals dilated ventricles
without obstruction. This condition is
often due to impaired absorption of CSF
by which anatomical structure?
A. Central canal
B. Choroid plexus
C. Arachnoid villi
D. Dural sinus valves
E. Foramen of Monro
89.
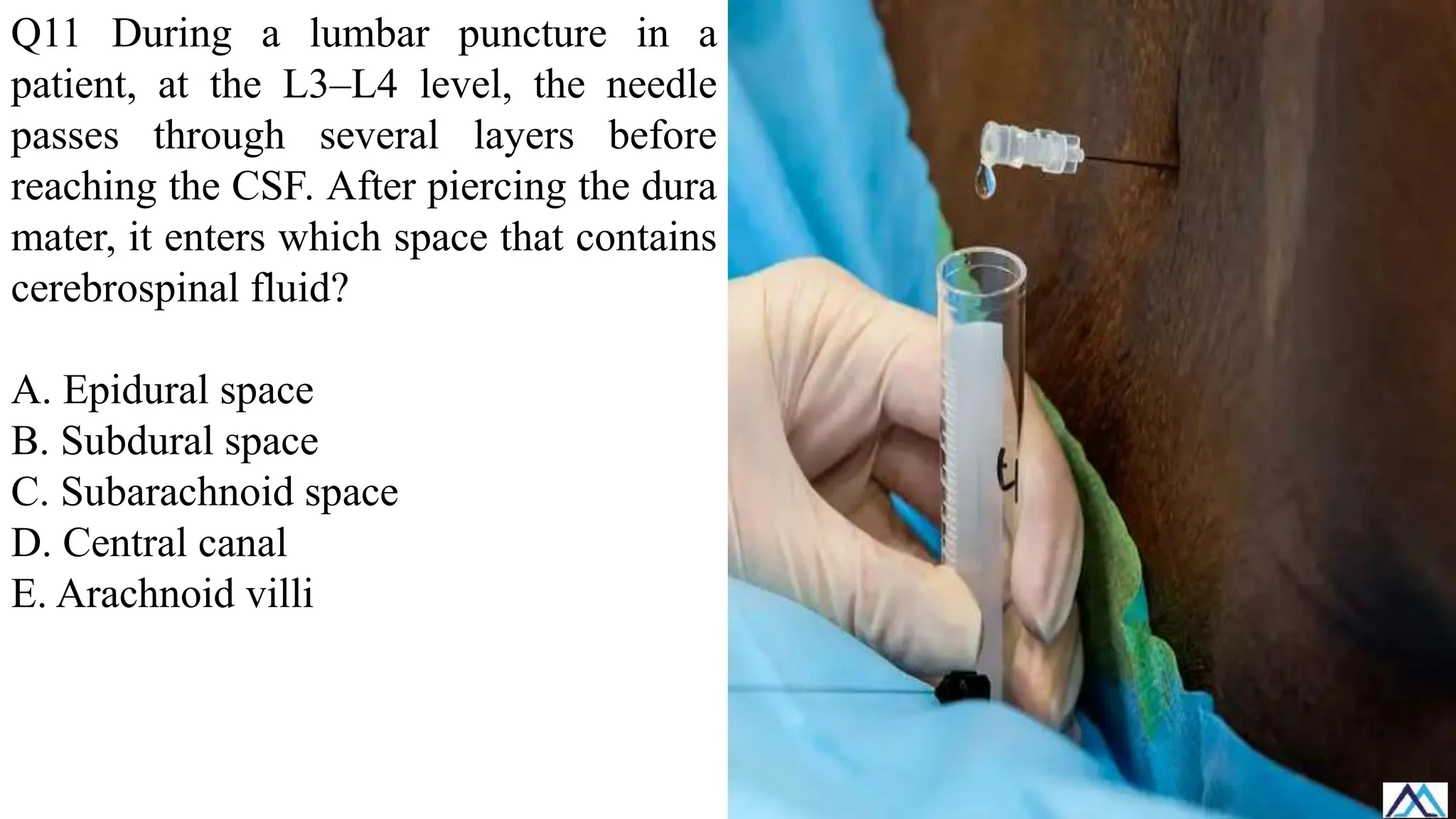
Q11 During alumbar puncture in a
patient, at the L3–L4 level, the needle
passes through several layers before
reaching the CSF. After piercing the dura
mater, it enters which space that contains
cerebrospinal fluid?
A. Epidural space
B. Subdural space
C. Subarachnoid space
D. Central canal
E. Arachnoid villi
90.
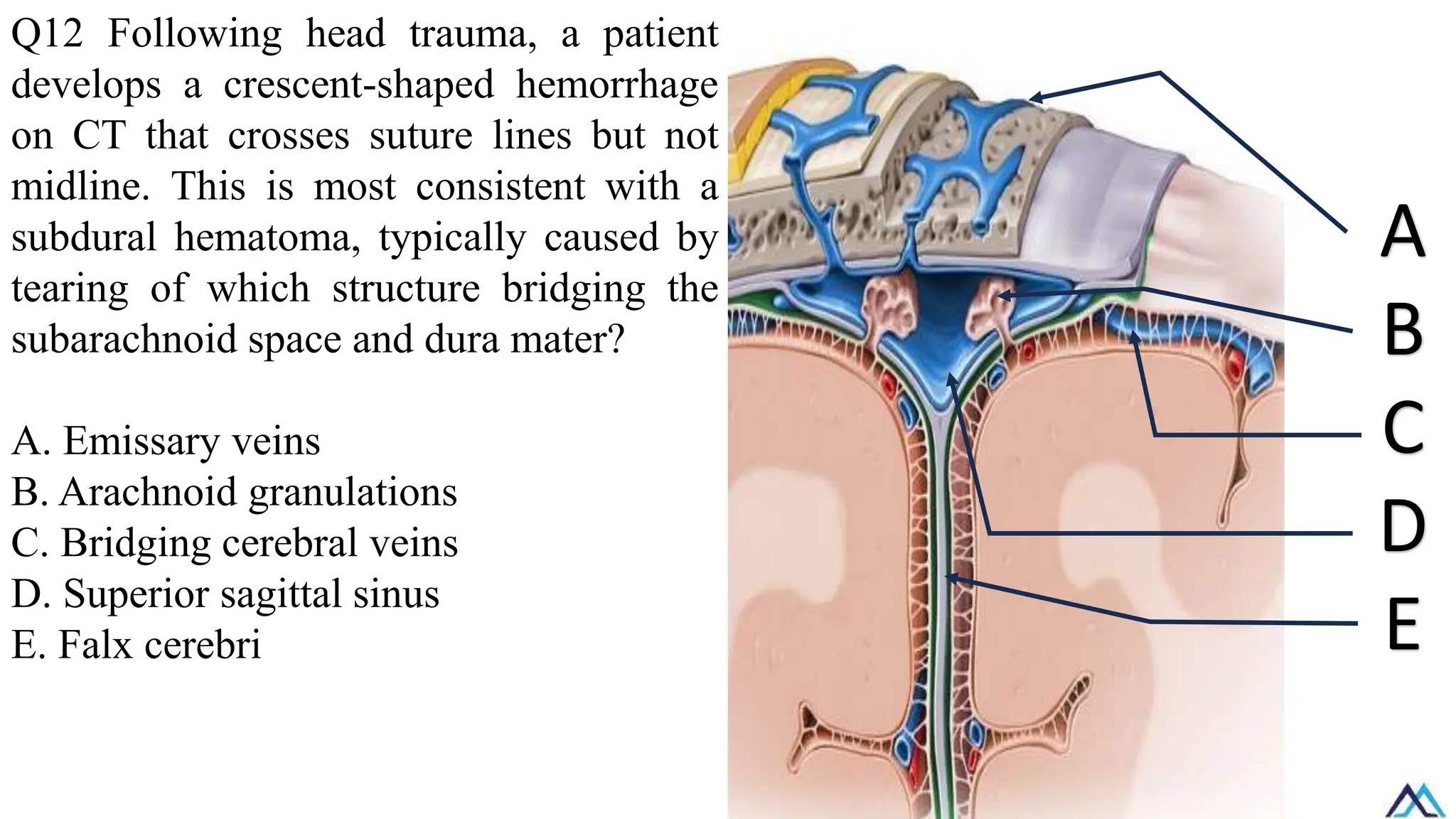
Q12 Following headtrauma, a patient
develops a crescent-shaped hemorrhage
on CT that crosses suture lines but not
midline. This is most consistent with a
subdural hematoma, typically caused by
tearing of which structure bridging the
subarachnoid space and dura mater?
A. Emissary veins
B. Arachnoid granulations
C. Bridging cerebral veins
D. Superior sagittal sinus
E. Falx cerebri
A
B
C
D
E
91.
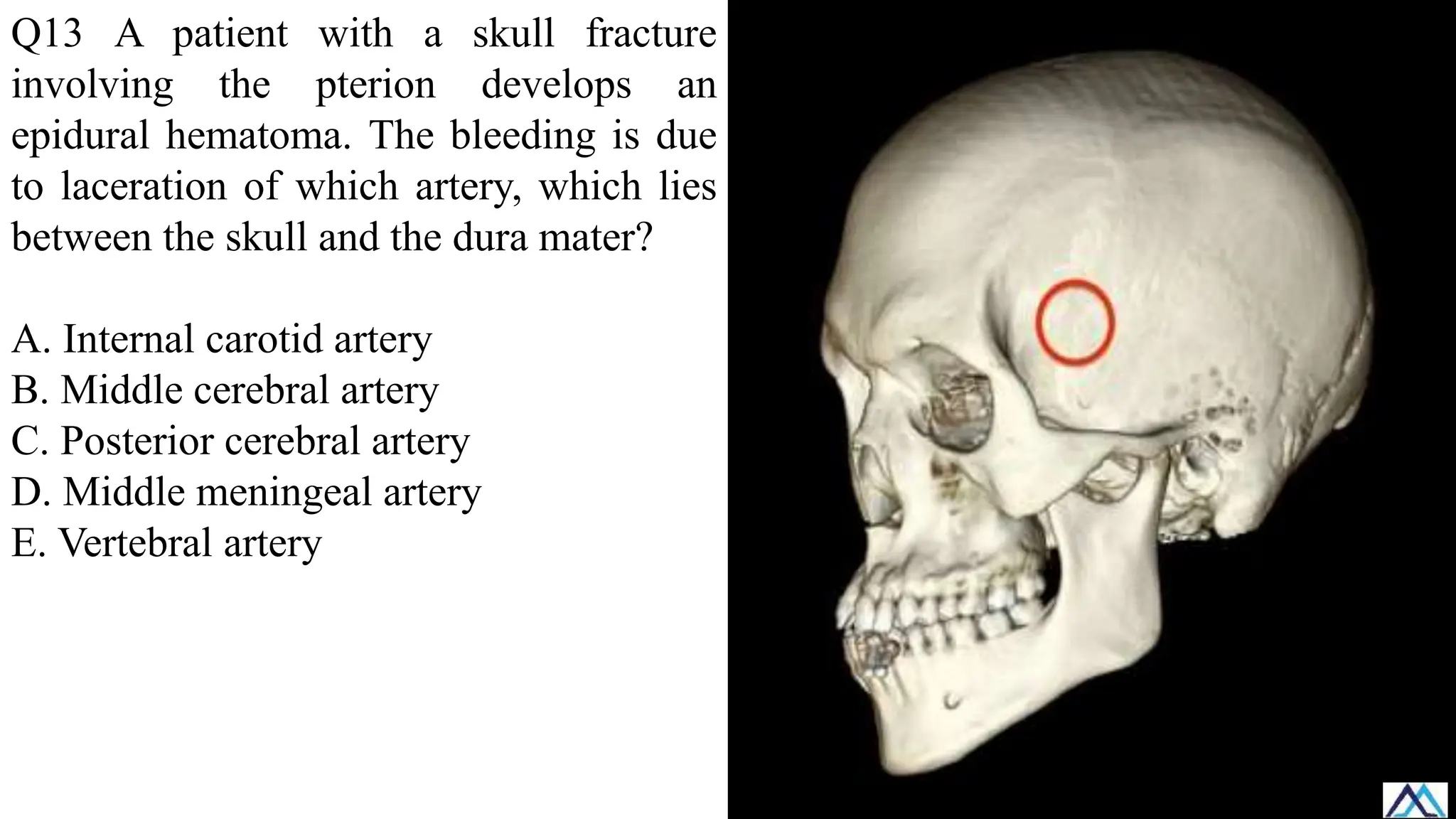
Q13 A patientwith a skull fracture
involving the pterion develops an
epidural hematoma. The bleeding is due
to laceration of which artery, which lies
between the skull and the dura mater?
A. Internal carotid artery
B. Middle cerebral artery
C. Posterior cerebral artery
D. Middle meningeal artery
E. Vertebral artery
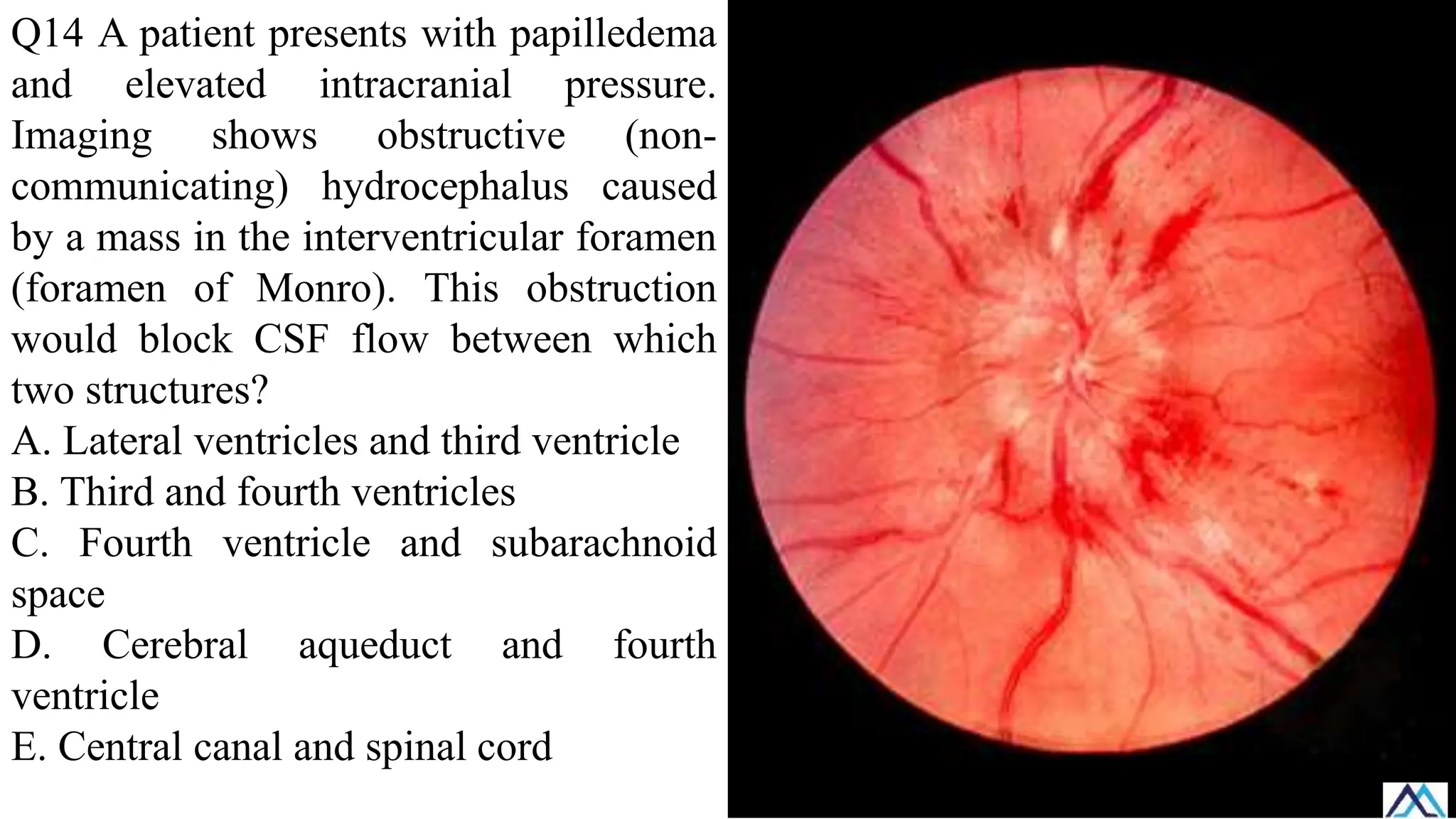
92.
Q14 A patientpresents with papilledema
and elevated intracranial pressure.
Imaging shows obstructive (non-
communicating) hydrocephalus caused
by a mass in the interventricular foramen
(foramen of Monro). This obstruction
would block CSF flow between which
two structures?
A. Lateral ventricles and third ventricle
B. Third and fourth ventricles
C. Fourth ventricle and subarachnoid
space
D. Cerebral aqueduct and fourth
ventricle
E. Central canal and spinal cord
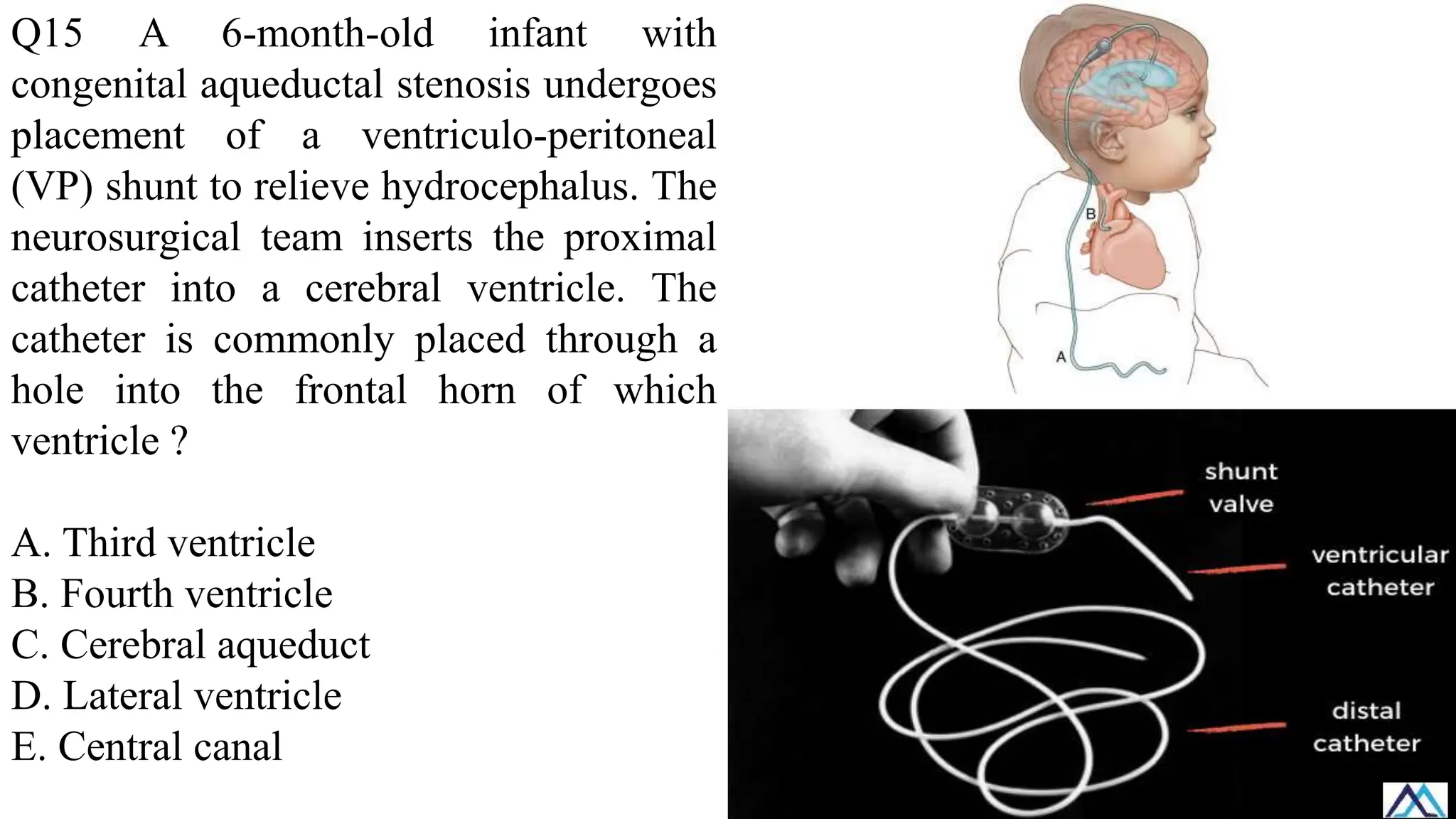
93.
Q15 A 6-month-oldinfant with
congenital aqueductal stenosis undergoes
placement of a ventriculo-peritoneal
(VP) shunt to relieve hydrocephalus. The
neurosurgical team inserts the proximal
catheter into a cerebral ventricle. The
catheter is commonly placed through a
hole into the frontal horn of which
ventricle ?
A. Third ventricle
B. Fourth ventricle
C. Cerebral aqueduct
D. Lateral ventricle
E. Central canal
Q1: The dura,arachnoid, and pia ------- are tightly connected with each other.
Q2: The denticulate ligaments attach -----entrances of the ventral and dorsal roots
Q3: Flow of cerebrospinal fluid is likely obstructed at the cerebral aqueduct.
Q4: Between L-3 and L-4.
Q5: Normal pressure hydrocephalus
Q6 The dura, arachnoid, and pia -------- tightly connected with each other.
Q7 Between L-4 and L-5
Q8 Arachnoid mater and pia mater
Q9 Subarachnoid space
Q10 Arachnoid villi
Q11 Subarachnoid space
Q12 Bridging cerebral veins
Q13 Middle meningeal artery
Q14 Lateral ventricles and third ventricle
Q15 Lateral ventricle
96.
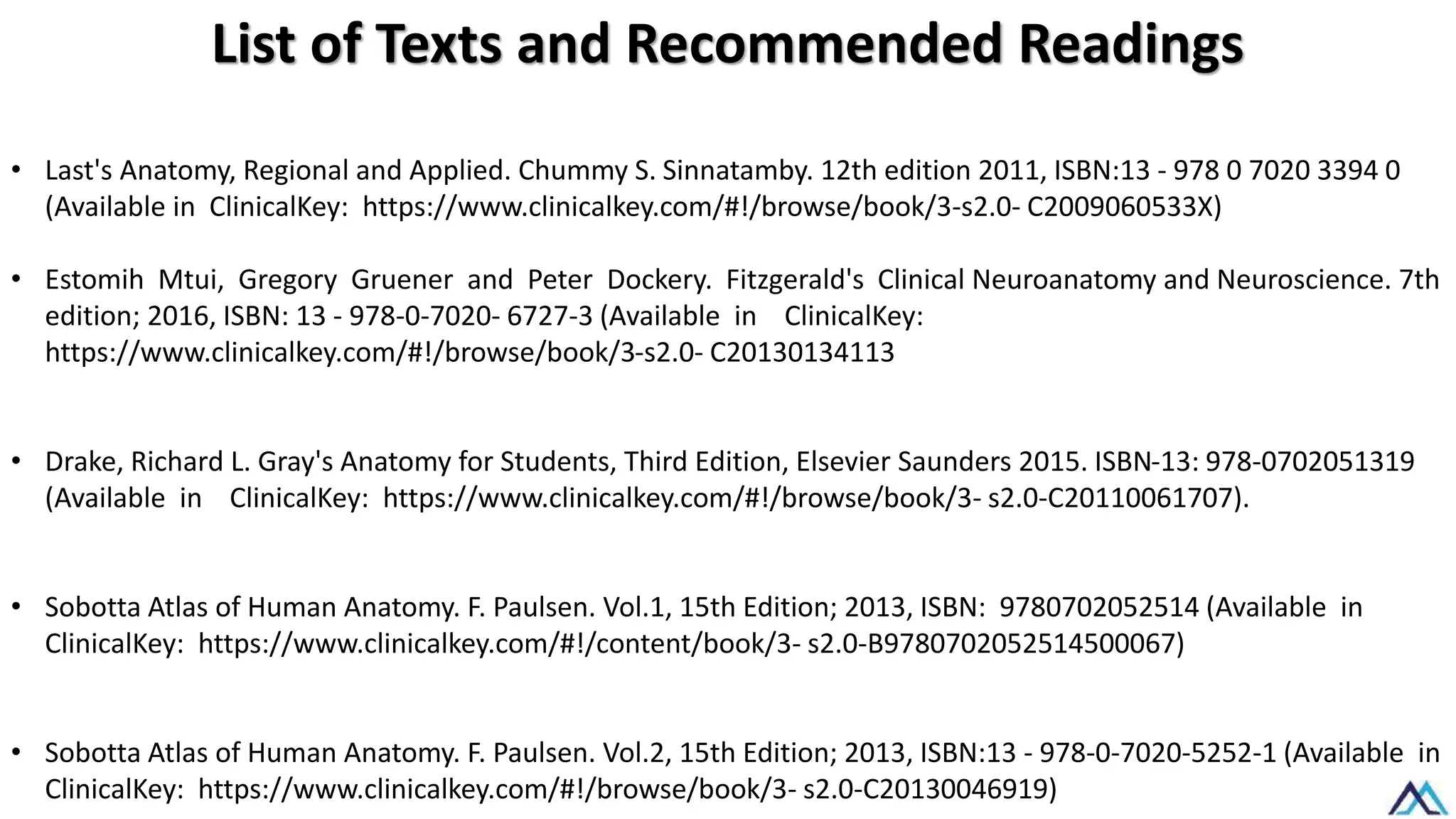
List of Textsand Recommended Readings
• Last's Anatomy, Regional and Applied. Chummy S. Sinnatamby. 12th edition 2011, ISBN:13 - 978 0 7020 3394 0
(Available in ClinicalKey: https://www.clinicalkey.com/#!/browse/book/3-s2.0- C2009060533X)
• Estomih Mtui, Gregory Gruener and Peter Dockery. Fitzgerald's Clinical Neuroanatomy and Neuroscience. 7th
edition; 2016, ISBN: 13 - 978-0-7020- 6727-3 (Available in ClinicalKey:
https://www.clinicalkey.com/#!/browse/book/3-s2.0- C20130134113
• Drake, Richard L. Gray's Anatomy for Students, Third Edition, Elsevier Saunders 2015. ISBN-13: 978-0702051319
(Available in ClinicalKey: https://www.clinicalkey.com/#!/browse/book/3- s2.0-C20110061707).
• Sobotta Atlas of Human Anatomy. F. Paulsen. Vol.1, 15th Edition; 2013, ISBN: 9780702052514 (Available in
ClinicalKey: https://www.clinicalkey.com/#!/content/book/3- s2.0-B9780702052514500067)
• Sobotta Atlas of Human Anatomy. F. Paulsen. Vol.2, 15th Edition; 2013, ISBN:13 - 978-0-7020-5252-1 (Available in
ClinicalKey: https://www.clinicalkey.com/#!/browse/book/3- s2.0-C20130046919)
![After 21 centuries of scientific inquiry,
our understanding of cellular biology
has made significant progress, but the
percentage of nervous system cells for
which we fully understand all
functions is indeed relatively low
[almost 10%]. The 90%, are still under
exploration.](https://image.slidesharecdn.com/020csfandmeninges-251127195153-16a12942/75/CSF-and-meninges-CSF-and-meninges-CSF-and-meninges-pdf-1-2048.jpg)