Proximal Gastrectomy With Double Tract Reconstruction.pptx
1.
Proximal Gastrectomy WithDouble Tract Reconstruction :
A Novel Approach
Dr. Anant Pore
Surgical Oncologist
2.
Epidemiology
● Worldwide, asteady decline in incidence.
● India comparing 2015 and 2020 is on the increasing trend.
● Majority of the countries show a proximal shift over the past two decades.
Servarayan Murugesan, J. (2018). Gastric cancer in India: epidemiology and standard of treatment. Updates in
Surgery, 70(2), 233–239. doi:10.1007/s13304-018-0527-3
3.
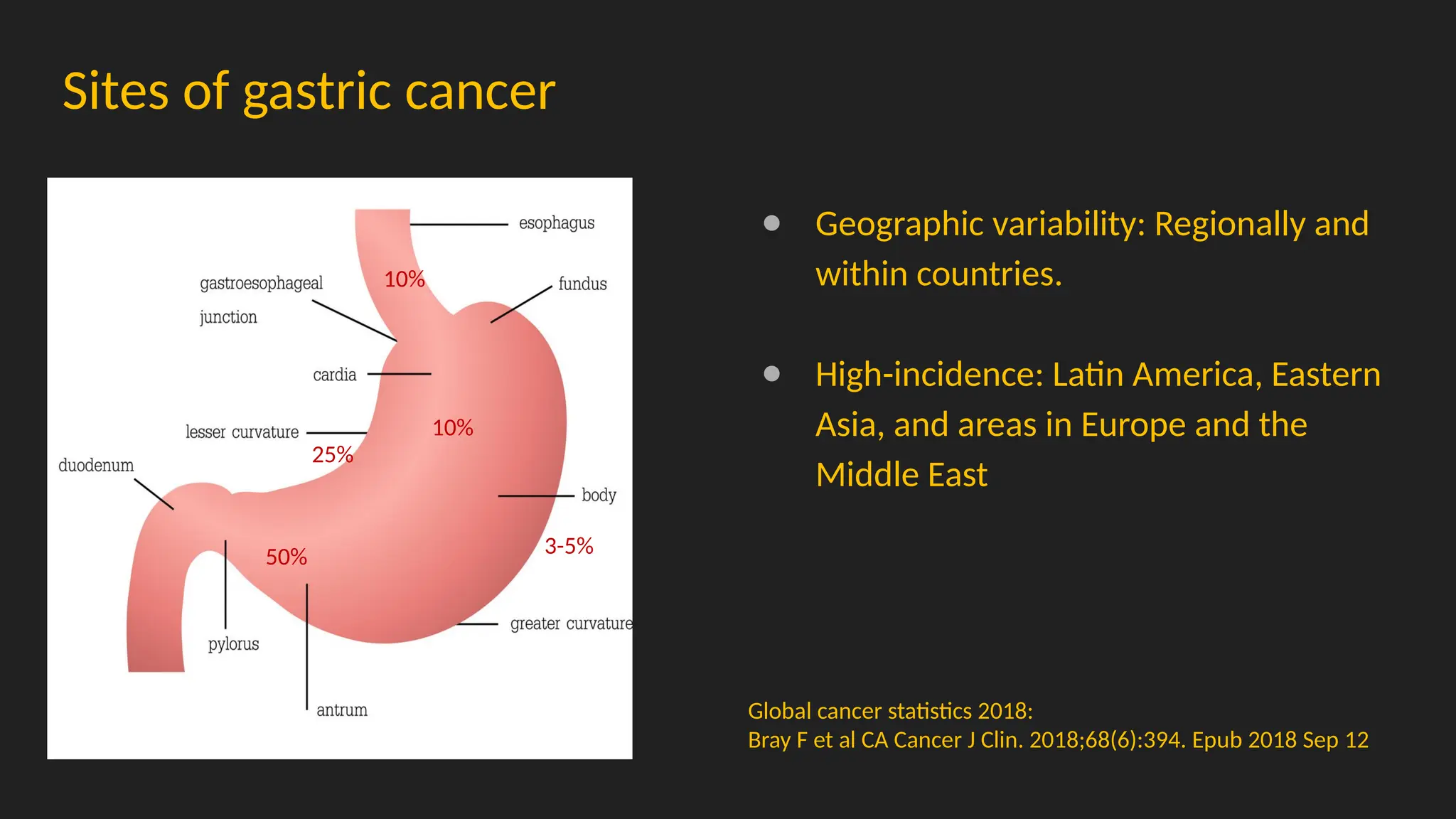
Sites of gastriccancer
● Geographic variability: Regionally and
within countries.
● High-incidence: Latin America, Eastern
Asia, and areas in Europe and the
Middle East
Global cancer statistics 2018:
Bray F et al CA Cancer J Clin. 2018;68(6):394. Epub 2018 Sep 12
10%
25%
50%
10%
3-5%
4.
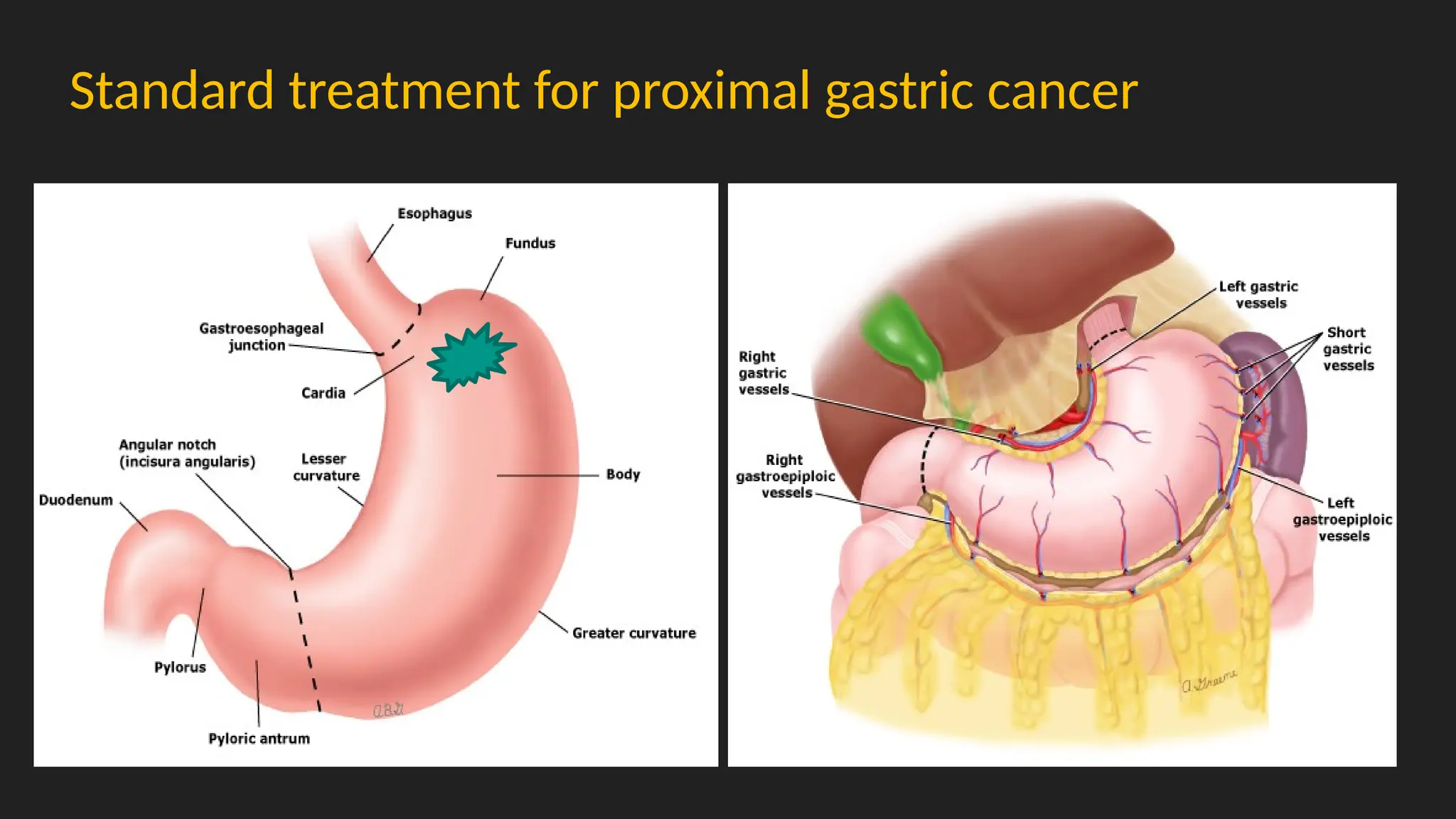
Standard surgery forgastric cancer
Perform
gastrectomy
with adequate
margins
Dissect
perigastric and
extragastric
lymph nodes
Conduct
gastrointestinal
reconstruction
afterward
5.
● Which patientsare oncological appropriate for proximal gastrectomy.
● Various type of reconstruction available after PG
● Benefits of PG vs TG
6.
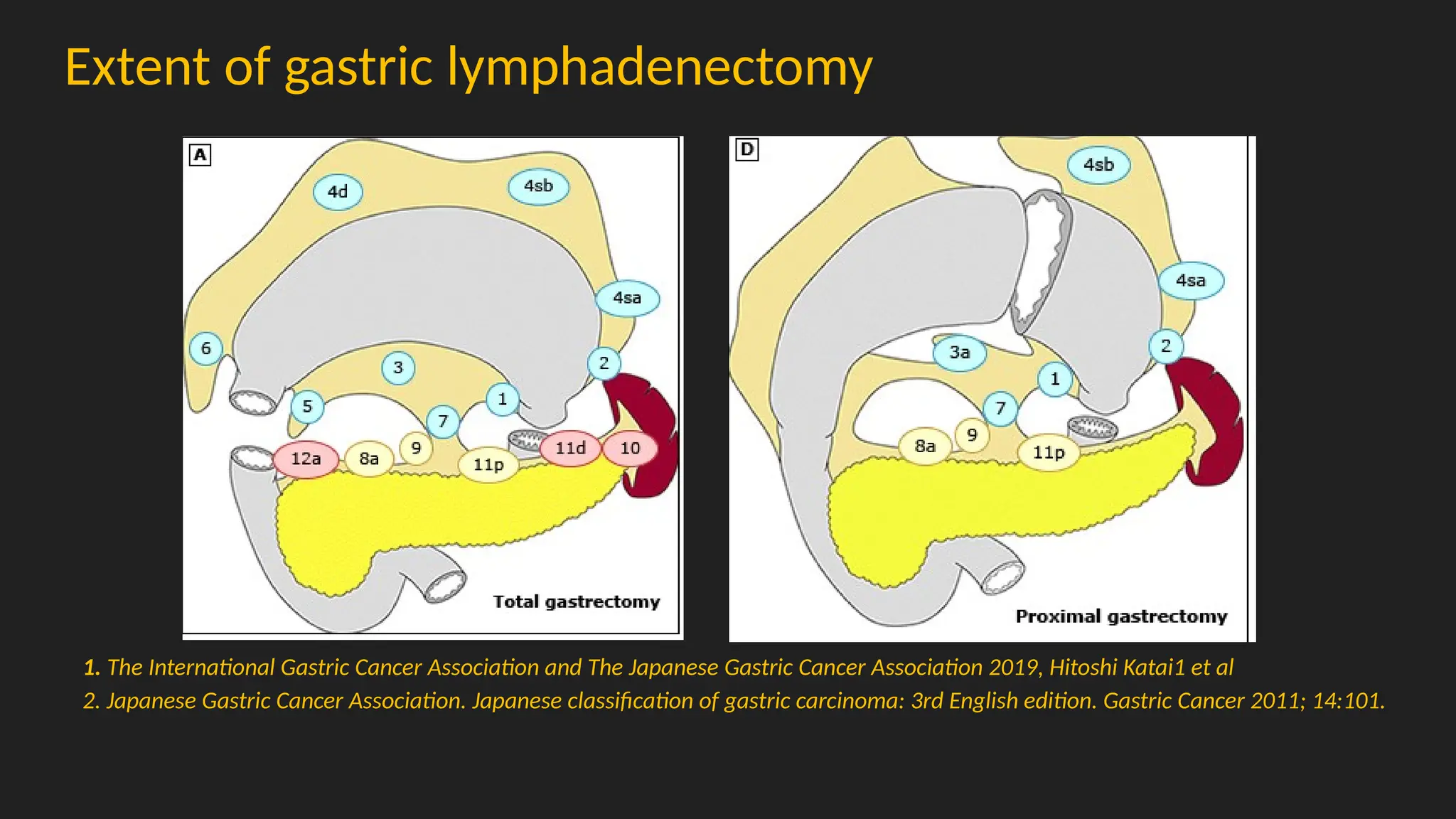
Extent of gastriclymphadenectomy
1. The International Gastric Cancer Association and The Japanese Gastric Cancer Association 2019, Hitoshi Katai1 et al
2. Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer 2011; 14:101.
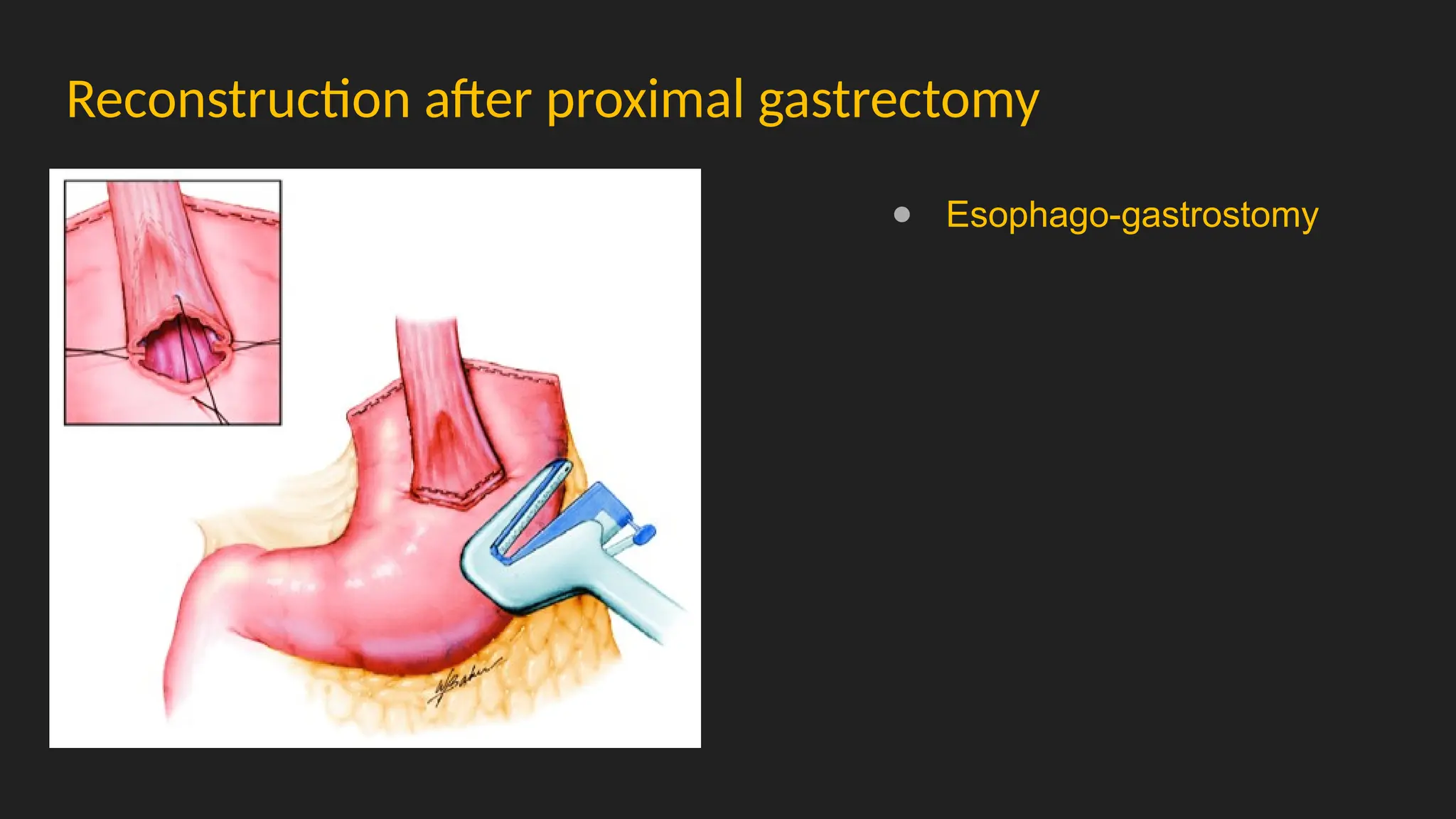
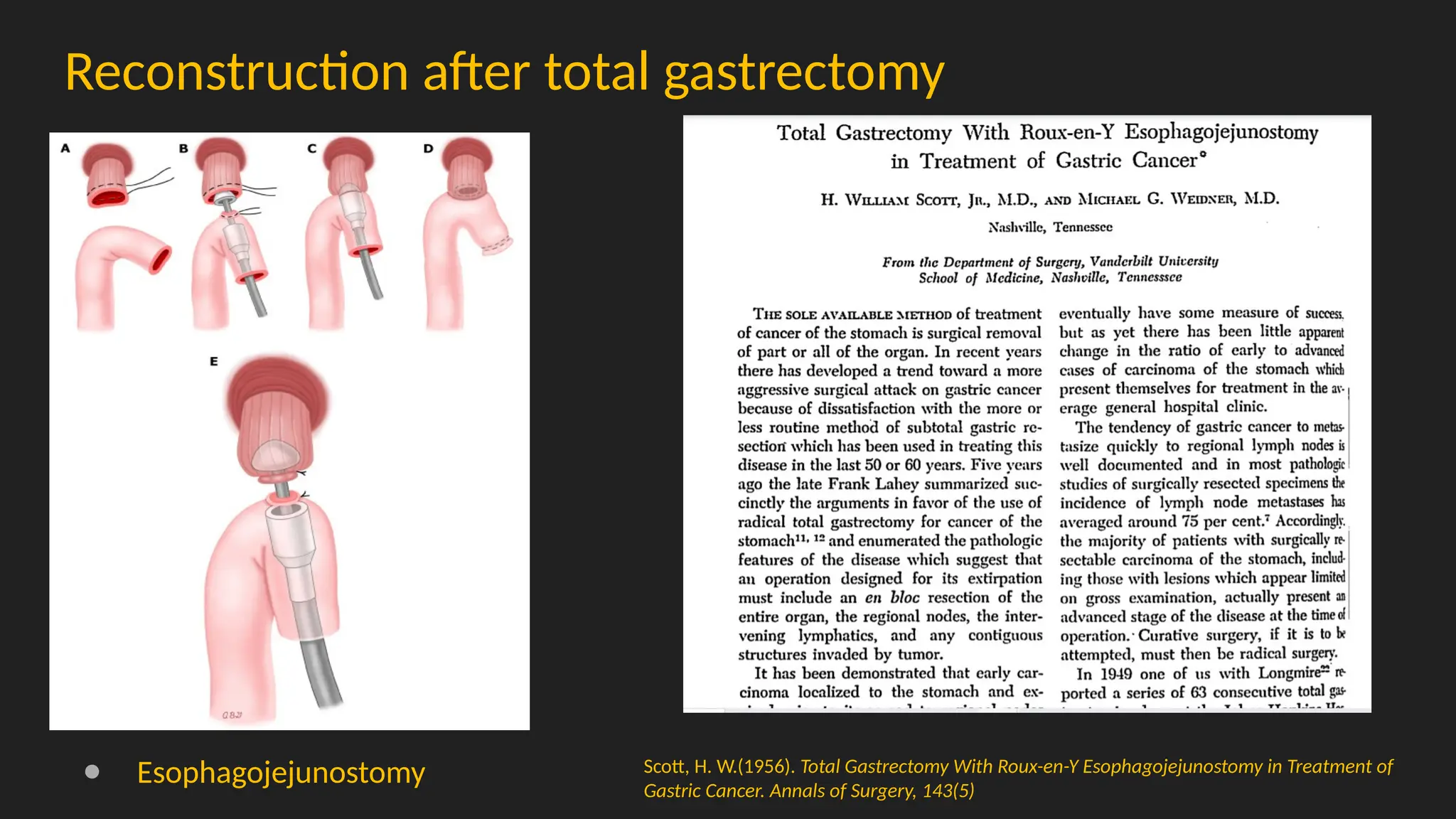
Reconstruction after totalgastrectomy
● Esophagojejunostomy Scott, H. W.(1956). Total Gastrectomy With Roux-en-Y Esophagojejunostomy in Treatment of
Gastric Cancer. Annals of Surgery, 143(5)
9.
Reconstruction after totalgastrectomy
Hunt-Lawrence type pouch
Pouch Versus No Pouch Following Total Gastrectomy: Meta-analysis of Randomized
and Non-randomized Studies.
Syn NL, Wee I, Shabbir A, Kim G, So JB
Ann Surg. 2019;269(6):1041.
o 17 RCT and 8 observational studies
o Decreased incidence of esophagitis &
heartburn (63% [RR]),
o Dumping syndrome (73% RR),
o Food intake disturbance (50% RR)
Post gastrectomy sequalae
●Gastric reservoir dysfunction
○ Metabolic aberrations and dumping syndrome
● Vagal denervation
○ Diarrhea, gastric stasis and gall stone
● Aberration in reconstruction
○ Bile reflux gastritis
○ Afferent and efferent loop obstruction
○ Roux stasis and jejuno-gastric intussusception
12.
Proximal gastrectomy forproximal tumours
● Immediate appeal of retaining some gastric reservoir
● Recent meta-analysis (1 RCT, 7 retrospective study)
Similar survival
Less local recurrence with total gastrectomy
High risk of reflux esophagitis and anastomotic stricture with proximal
gastrectomy
Hepatogastroenterology. 2012 Mar-Apr;59(114):633-40
The International Gastric Cancer Association and The Japanese Gastric Cancer Association 2019, Hitoshi Katai1 et
al
13.
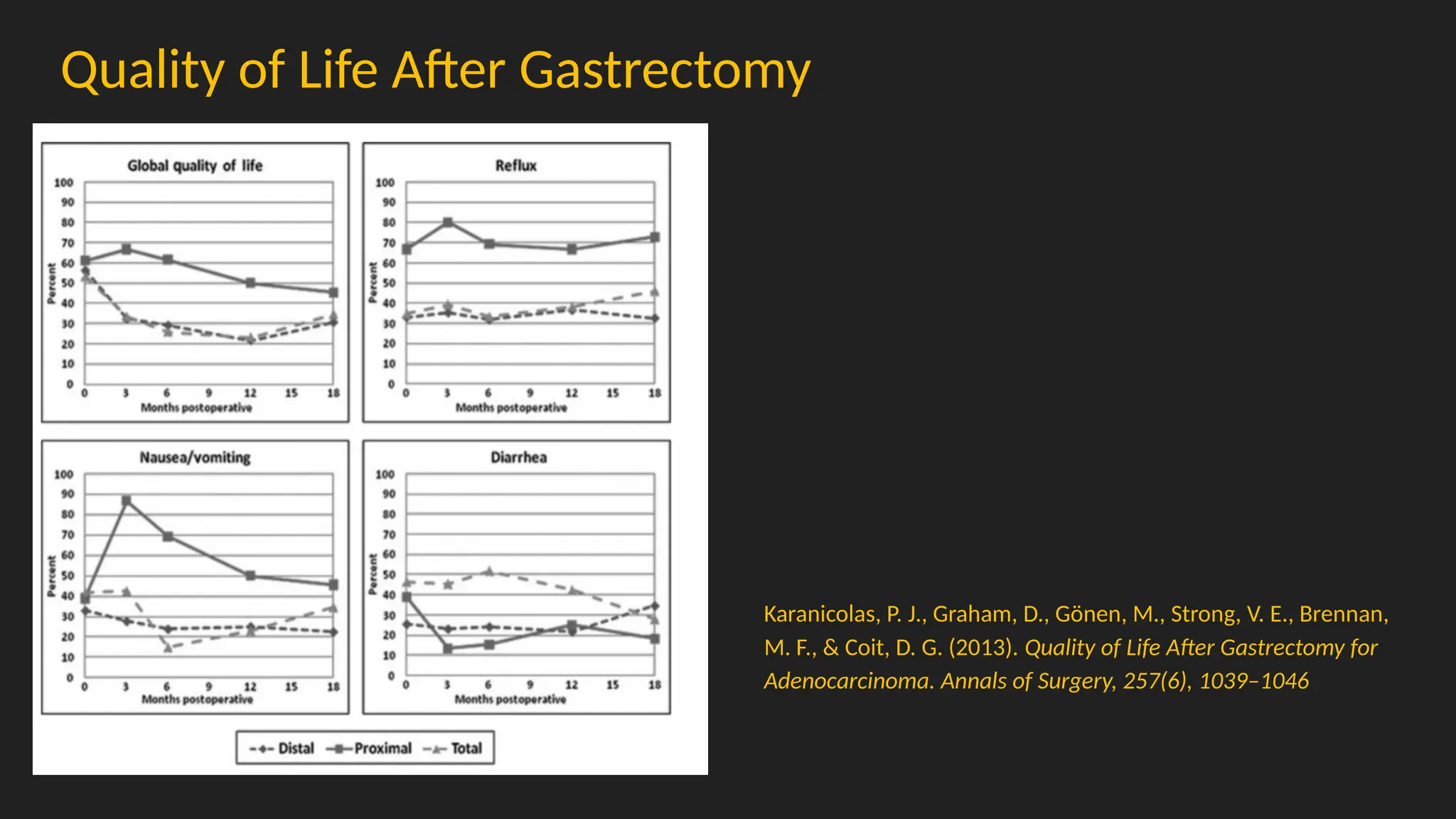
Quality of LifeAfter Gastrectomy
Karanicolas, P. J., Graham, D., Gönen, M., Strong, V. E., Brennan,
M. F., & Coit, D. G. (2013). Quality of Life After Gastrectomy for
Adenocarcinoma. Annals of Surgery, 257(6), 1039–1046
14.
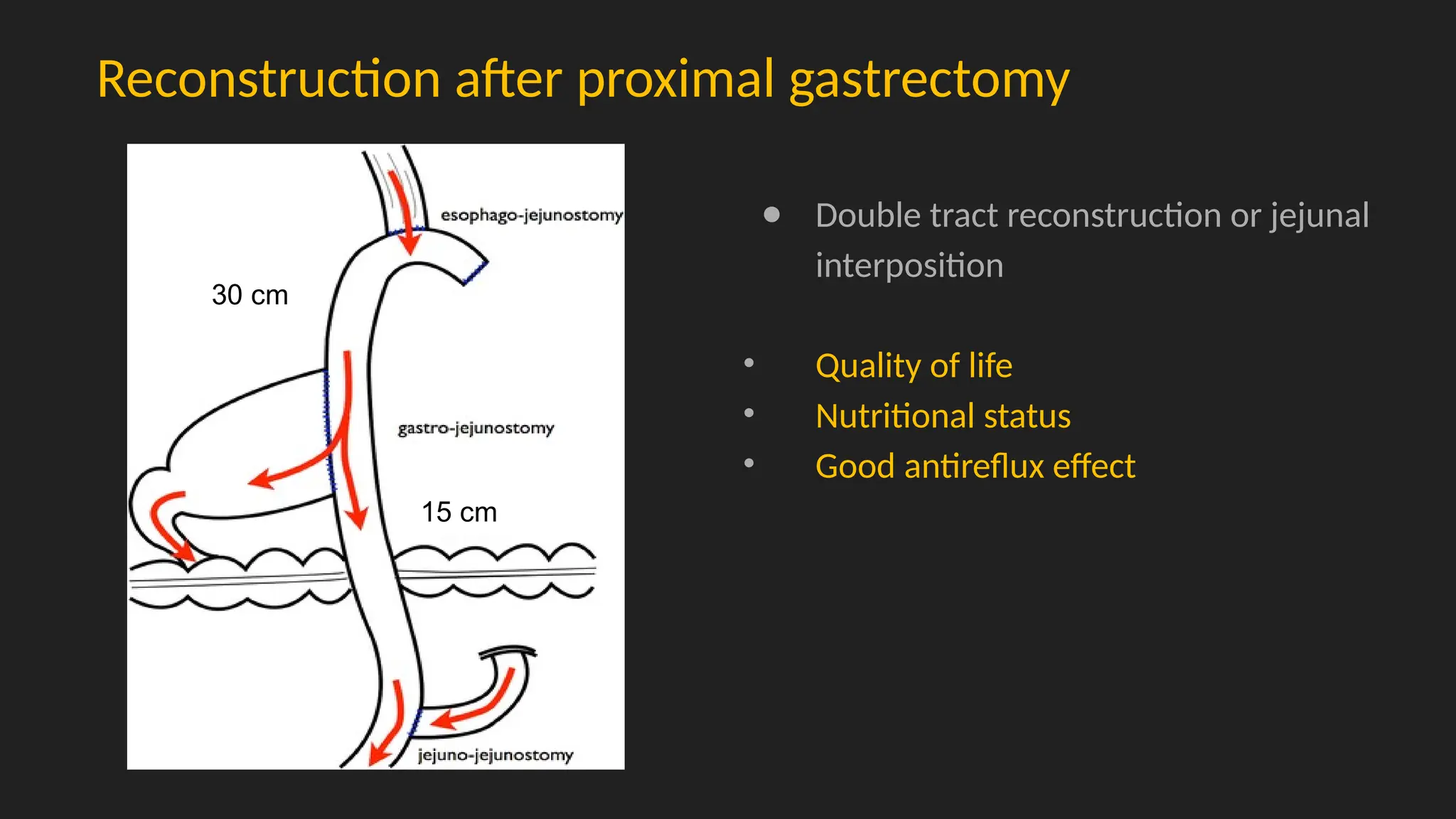
Reconstruction after proximalgastrectomy
● Double tract reconstruction or jejunal
interposition
• Quality of life
• Nutritional status
• Good antireflux effect
30 cm
15 cm
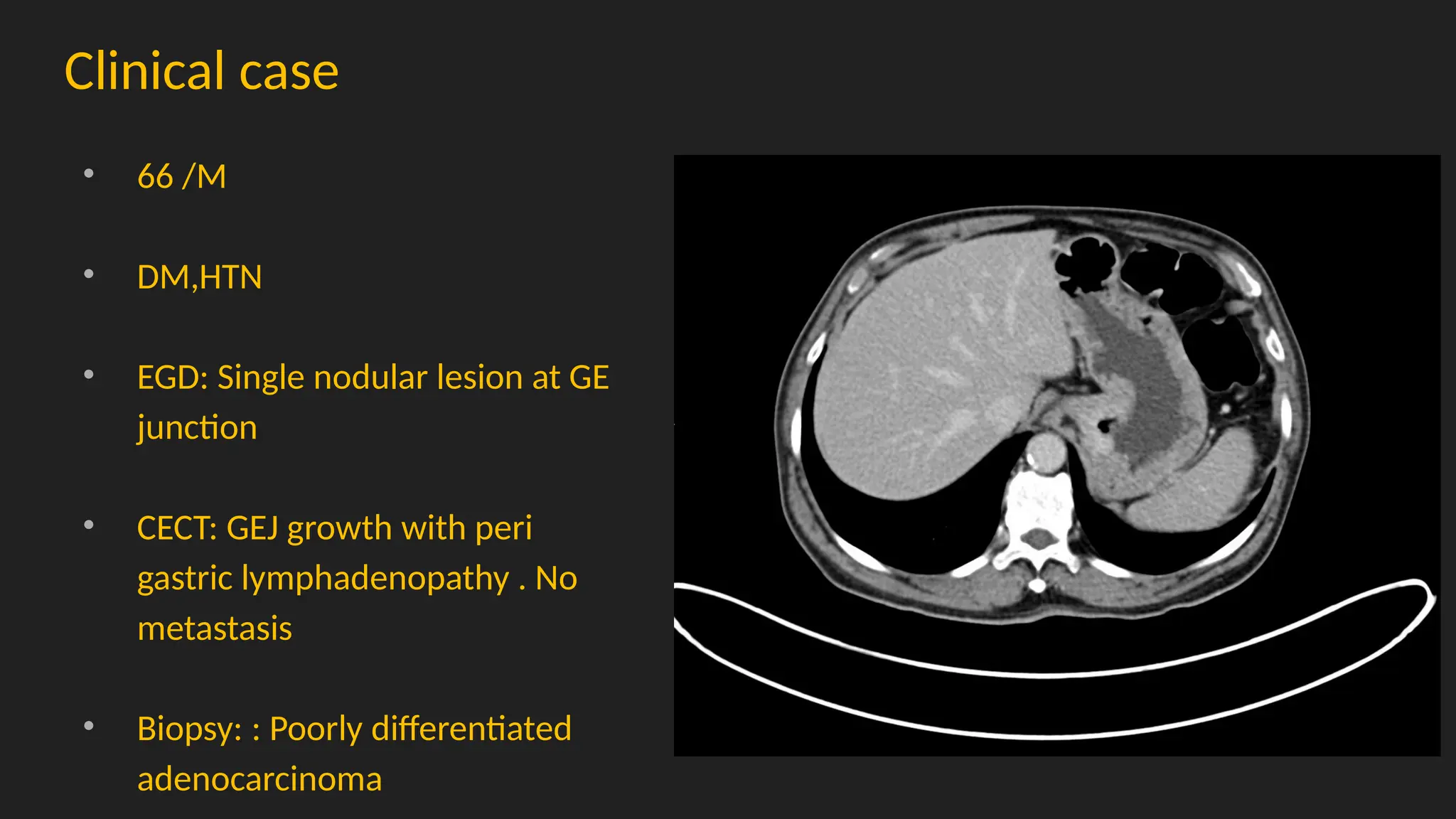
Clinical case
• 66/M
• DM,HTN
• EGD: Single nodular lesion at GE
junction
• CECT: GEJ growth with peri
gastric lymphadenopathy . No
metastasis
• Biopsy: : Poorly differentiated
adenocarcinoma
Post op
● POD1: Freka feeding started (Perioperative nutrition)
● POD 7: Oral liquid diet gradually progressed to normal diet (post gastrectomy diet)
● POD 7: Gastrograffin study- no leak and stenosis
20.
Histology
SIGNET RING CELLCARCINOMA, DIFFUSE TYPE, POORLY DIFFERENTIATED.
- The tumour is unifocal, located in the fundus and measures 4 cm in maximum dimension, grossly.
- Tumor penetrates the subserosal connective tissue and invades the serosa (visceral peritoneum) focally.
- Lymphovascular invasion is present and Perineural invasion is present.
- The proximal and distal margins are free of tumour, grossly and microscopically. The proximal margin is 0.8 cm away from the
tumour and distal margin is 4.5 cm away from the tumour, grossly.
- The adjacent gastric mucosa does not show any significant histopathological changes.
- Lymph node 11/36
- pT4aN3a (Staged as per UICC/AJCC 8th edition)
21.
Patience – Passion– Consistency
Consistency is what transforms average into excellence
Editor's Notes
#2
Gastric cancer remains a major cause of cancer-related mortality worldwide. Shifts in the distribution of anatomical locations have been detected in several high-incidence regions. Globally, gastric cancer remains the fifth most common malignant cancer and the fourth leading cause of cancer-related mortality. Despite declining incidence rates, the global burden of this malignancy is expected to have a 62% increase by 2040. Worldwide, Helicobacter pylori infection accounts for almost 90% of distal gastric cancers; other well-established risk factors include excess body fat, cigarette smoking and diets high in salt and processed meats.
#3 Majority of the countries show a proximal shift of gastric cancer over the past two decades.
Our study concluded that there was no proximal shift in Indian populations over four decades.
#7 Partial gastrectomy (distal gastrectomy, subtotal gastrectomy) (figure 1) with resection of adjacent lymph nodes appears to be sufficient for lesions in the distal (lower two-thirds) of the stomach
The issues guiding the extent of surgical resection are more complex for tumors of the proximal stomach.
Total gastrectomy (figure 2), which removes the entire stomach, remains the preferred treatment for most proximal gastric cancers
Proximal gastrectomy resects the cardia and upper portion of the corpus, but more than half of the stomach remains (figure 3). Proximal gastrectomy is intended for early gastric cancer (cT1) that is not amenable to endoscopic resection and is usually performed in Eastern countries where such early-stage diseases are prevalent, but not commonly in Western countries. Although esophagogastrostomy after proximal gastrectomy may be a simple and safe reconstruction technically, it can lead to a high incidence of reflux esophagitis and impair postoperative quality of life.
#8 This article, published in 1956, highlights that people were performing similar surgeries 80 years ago as we do today. However, it’s important to note that surgical techniques have undergone significant modifications, and advancements in chemotherapy molecules have greatly enhanced surgical outcomes. Here, we discuss the simplest technique for total gastrectomy and the continuity of the gastrointestinal tract.
#9 a Hunt-Lawrence type pouch with a Roux-en-Y reconstruction
#10 D1,D2,D3
Simple esophagogastrostomy after PG /TG is the simplest and most convenient physiological reconstruction method. Without additional antireflux reconstruction.
#12 . Alternative to proximal gastrectomy is a total gastrectomy Compared with total gastrectomy, proximal gastrectomy may have nutritional benefits but a higher incidence of bile reflux and anastomotic stenosis. The exact balance between the advantages and disadvantages of proximal gastrectomy lies in its reconstruction [
Esophagogastrostomy –
Jejunal interposition
Double-tract reconstruction
. In a meta-analysis of one trial and 13 nonrandomized studies comparing proximal gastrectomy with double-tract reconstruction with total gastrectomy, the former was associated with superior nutritional outcomes, but oncologic equivalency could not be assessed due to potential selection bias against total gastrectomy [45]. The randomized trial reported very few tumor recurrences [46]. The KLASS-05 trial also found laparoscopic proximal gastrectomy with double-tract reconstruction and laparoscopic gastrectomy comparable in perioperative outcomes [
#14 etsuo Maki (Tohoku University) introduced "Pylorus preserving gastrectomy" in 1967.
Procedure aimed to reduce dumping syndrome, postgastrectomy gallstones, and digestive issues after distal gastrectomy for benign ulcers.
Tsuneo Shiratori (Nara Medical University) expanded the procedure's use to gastric cancer treatment in 1991.
![Reconstruction after total gastrectomy
Hunt-Lawrence type pouch
Pouch Versus No Pouch Following Total Gastrectomy: Meta-analysis of Randomized
and Non-randomized Studies.
Syn NL, Wee I, Shabbir A, Kim G, So JB
Ann Surg. 2019;269(6):1041.
o 17 RCT and 8 observational studies
o Decreased incidence of esophagitis &
heartburn (63% [RR]),
o Dumping syndrome (73% RR),
o Food intake disturbance (50% RR)](https://image.slidesharecdn.com/proximalgastrectomywithdoubletractreconstruction-251127174031-ccc546bf/75/Proximal-Gastrectomy-With-Double-Tract-Reconstruction-pptx-9-2048.jpg)