Investigation
Depends onthe demographic profile, history
and clinical examination (systemic and ocular)
Detailed investigations is not required in all
cases
In anterior uveitis, investigations required if
Bilateral involvement
Recurrent episodes
Systemic association
Severe disease leading to significant loss of visual function
Indication:
• Rule out infection
• Specific therapy
• Systemic disease
• Whole management
Additional Investigation
Sarcoidosis– chest X-Ray, S. ACE, S. Calcium, HRCT
Tuberculosis – HRCT, Sputum examination, Lymph node biopsy
JRA - Rheumatoid factor, ANA
Syphilis - FTA-ABS
Wegeners granulomatosis - Antineutrophilic cytoplasmic Ab
Toxoplasmosis - Antitoxoplasma Ab
SLE – ANA
Behcets disease – HLA B51
Parasitic disease - Stool examination
9.
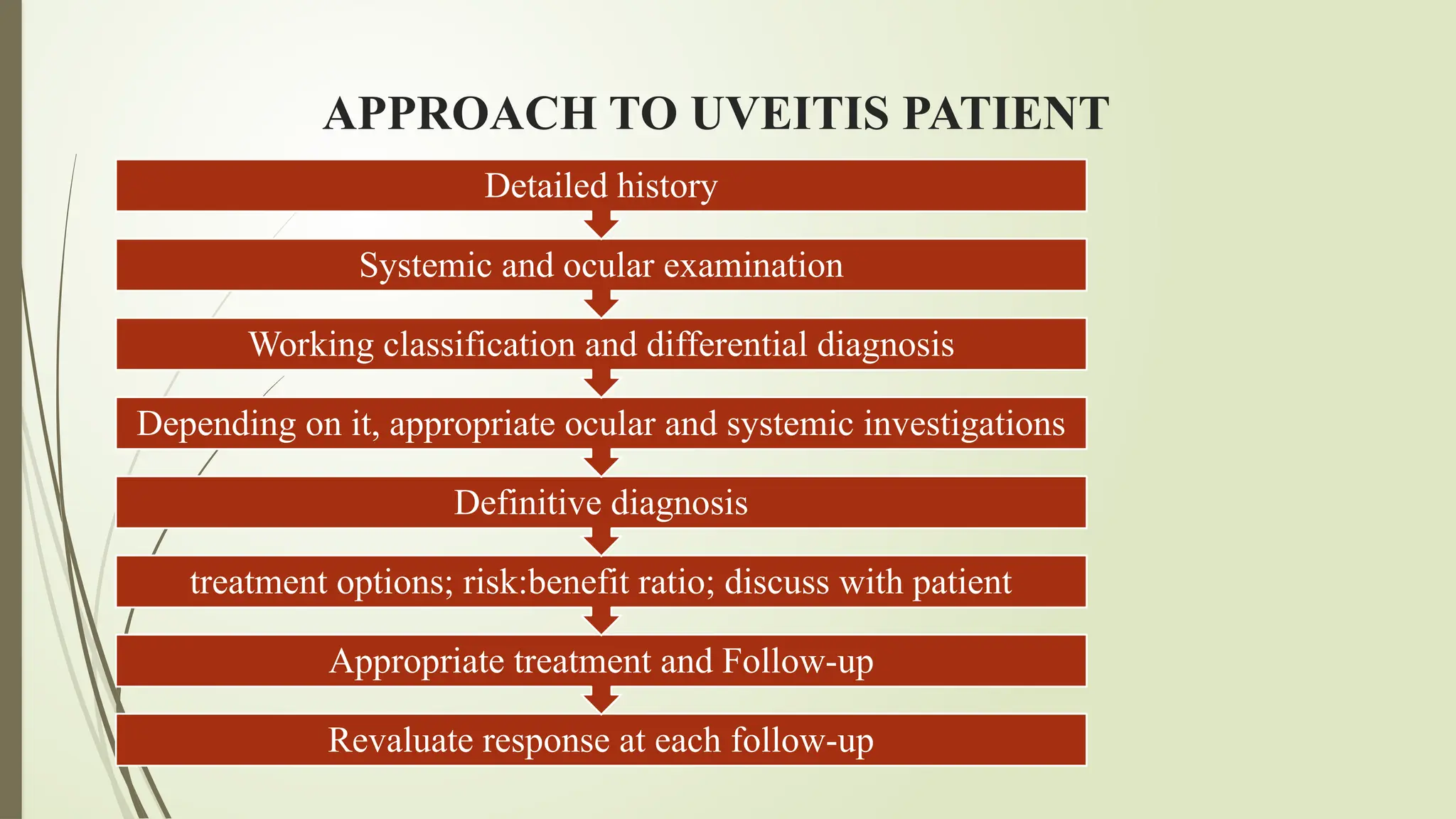
APPROACH TO UVEITISPATIENT
Revaluate response at each follow-up
Appropriate treatment and Follow-up
treatment options; risk:benefit ratio; discuss with patient
Definitive diagnosis
Depending on it, appropriate ocular and systemic investigations
Working classification and differential diagnosis
Systemic and ocular examination
Detailed history
10.
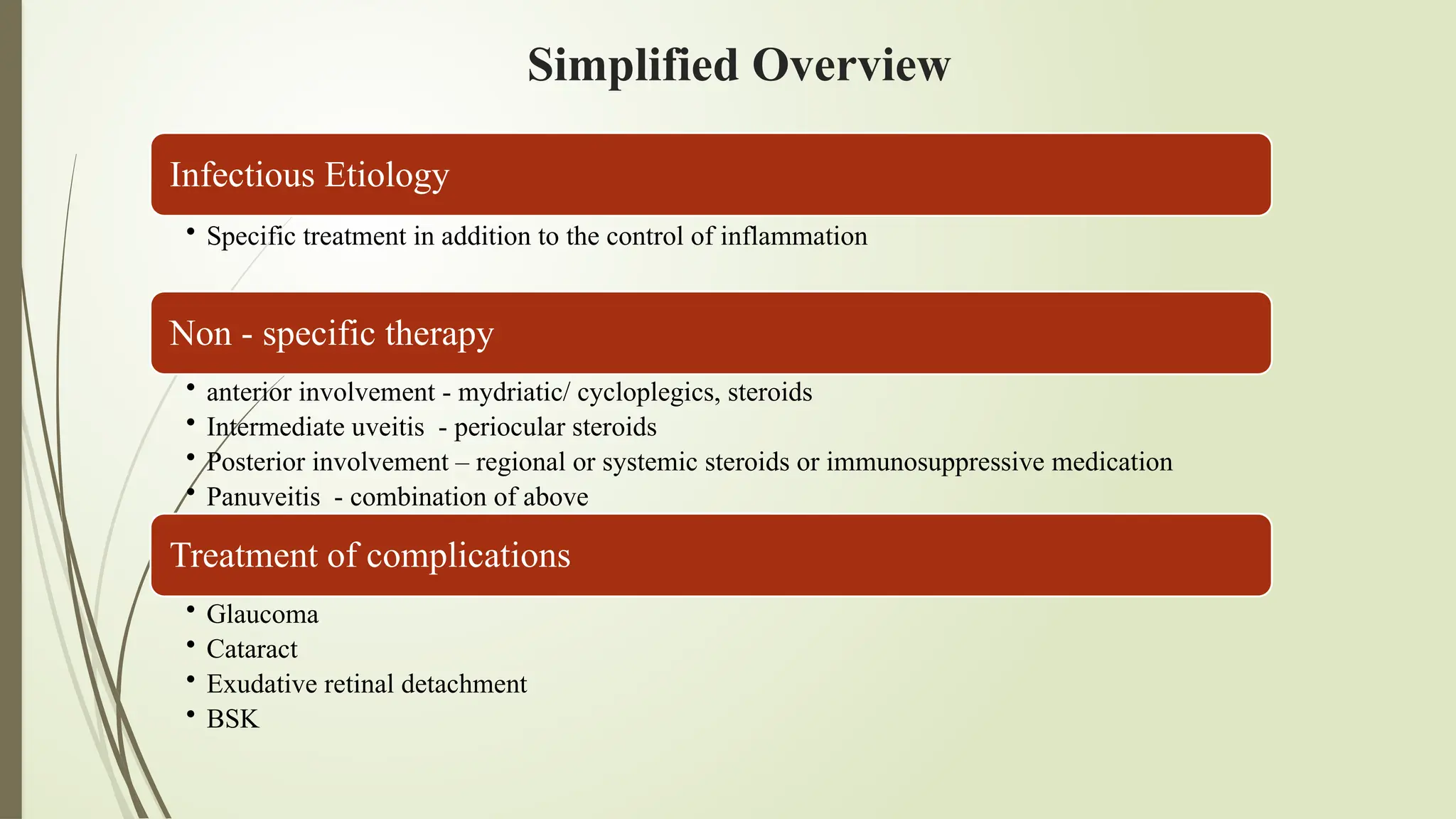
Simplified Overview
Infectious Etiology
•Specific treatment in addition to the control of inflammation
Non - specific therapy
• anterior involvement - mydriatic/ cycloplegics, steroids
• Intermediate uveitis - periocular steroids
• Posterior involvement – regional or systemic steroids or immunosuppressive medication
• Panuveitis - combination of above
Treatment of complications
• Glaucoma
• Cataract
• Exudative retinal detachment
• BSK
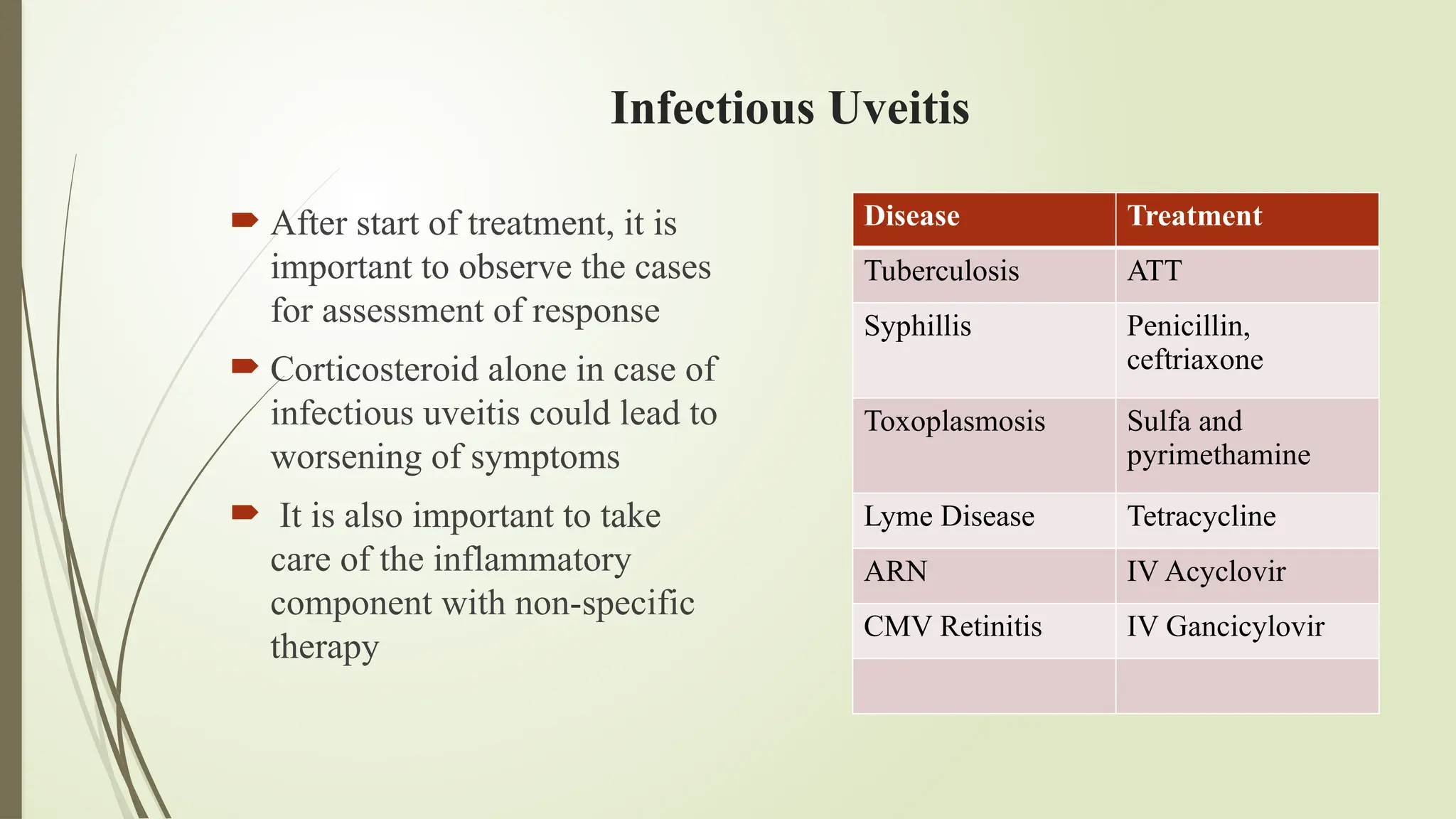
After startof treatment, it is
important to observe the cases
for assessment of response
Corticosteroid alone in case of
infectious uveitis could lead to
worsening of symptoms
It is also important to take
care of the inflammatory
component with non-specific
therapy
Disease Treatment
Tuberculosis ATT
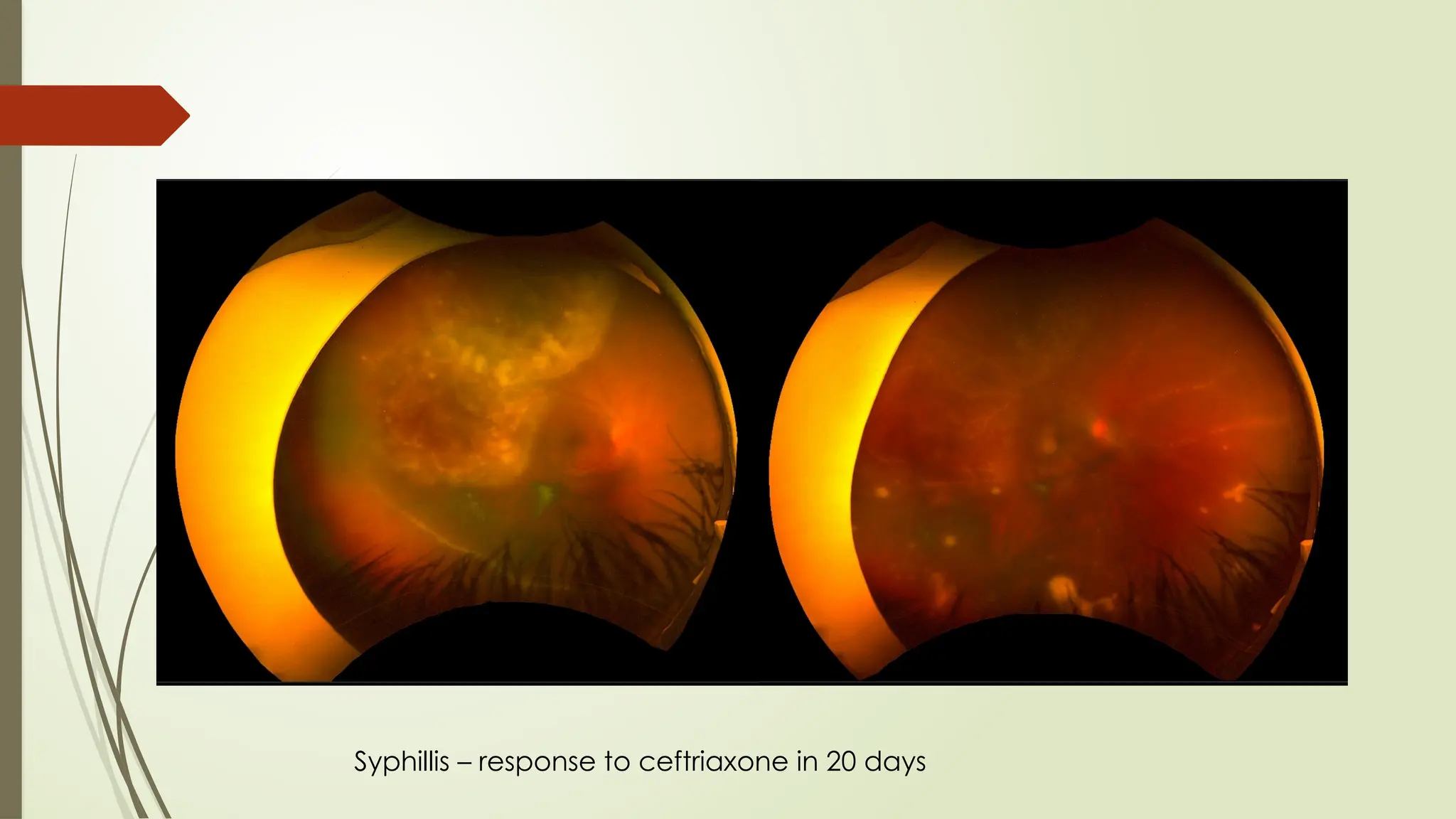
Syphillis Penicillin,
ceftriaxone
Toxoplasmosis Sulfa and
pyrimethamine
Lyme Disease Tetracycline
ARN IV Acyclovir
CMV Retinitis IV Gancicylovir
Infectious Uveitis
13.
Mydriatic/ Cycloplegics
Torelieve ciliary spasm and pain associated
Addition of a short acting agent prevent post. synechiae formation
To break down recently formed synechiae with intensive topical mydriatics
(atropine, phenylephrine)
Tropicamide 3-6 hrs
Cyclopentolate 18-30 hrs
Homatropine 18-36 hr
Atropine 10-14 days
14.
Steroids
Glucocorticoids exerta variety of immunosuppressive, anti-inflammatory and
anti-allergic effects on primary and secondary immune cells and tissues
Always start with higher dose and taper before stopping
Sinha A, Bagga A. Pulse steroid therapy. The Indian Journal of Pediatrics. 2008 Oct;75(10):1057–66.
Topical
Periocular
Intravitreal
Oral
Intravenous
15.
Steroids
Especially usefulin anterior segment
inflammation
Various preparations available
Action – ability to penetrate cornea;
relative anti-infl potency; duration of
action; dosage and frequency; SE
profile
Taper drug according to the response
Slow tapering especially with
recurrent attacks
IOP, HSV reactivation
Topical
16.
Steroids
Posterior involvement
Severe inflammation, unilateral disease
Especially in cases with CME
max dose to eye; minimal in systemic
Superotemporal area preferred
SE – perforation, proptosis, fibrosis, severe intractable
glaucoma
Effect last for 4-6 weeks
Avoided in steroid responders, glaucoma
Periocular
17.
Steroids
Intravitreal
Bypass blood-ocularbarrier; high
intraocular concentrations
Especially in cases with frequent
recurrence
April 2005 – Fuocinolone acetonide –
FDA appr chronic NI intermediate and
posterior uveitis
Ozurdex – Dexamethasone 700 ug implant
- FDA appr drug for NI posterior uveitis
Effect last for 3-6 months
18.
Steroids
Bilateral intermediateuveitis
Unilateral intermediate uveitis not responding
to PST
Posterior involvement and panuveitis with
Severe inflammation
Exudative retinal detachment
Rapid loss of vision
Lesion threatening macula, papillomacular
bundle or optic nerve
Systemic
IMMUNOSUPPRESSION
Before consideringimmunosuppression, one should
Patients adherence to treatment
reconsider diagnosis
Rule out tuberculosis, infections
Rule out liver, renal or hematological abnormalities
Meticulous follow-up available
Informed consent
Adverse reaction can be severe and life threatening
Delay in therapeutic response for weeks to months; therefore, need to be maintained
on corticosteroids until the immunomodulatory agent begins to take effect
25.
IMMUNOSUPPRESSION
INDICATION –
CS resistantor intolerant cases
Increase in inflammation when dose > 0.5mg/kg/day (30 mg/day) or
recurrence when the dose is decreased to < 7-10 mg/ day
In vision threatening inflammation, can be started as first line
Specific cases
Behcet disease
Sympathetic Ophthalmia
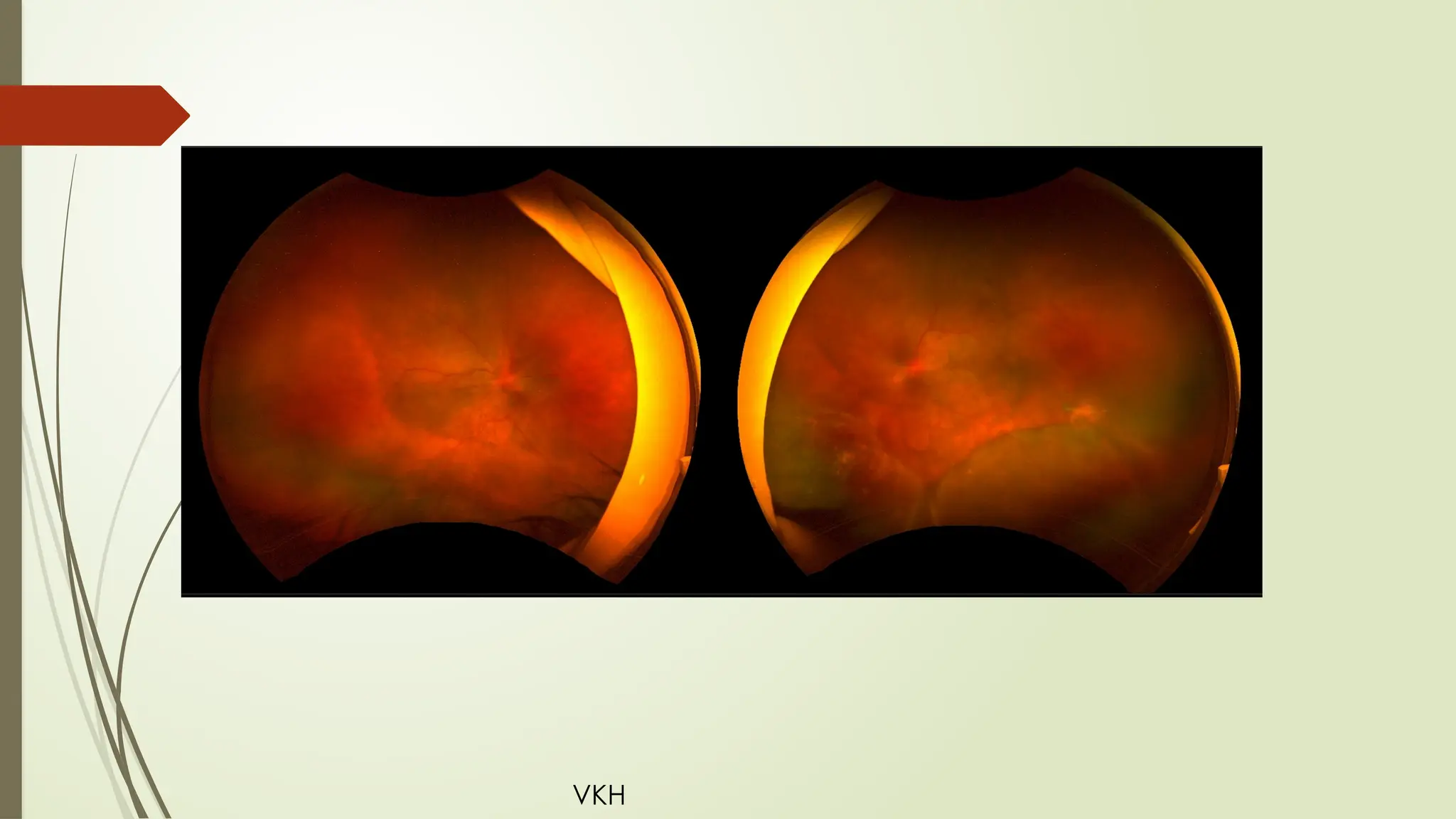
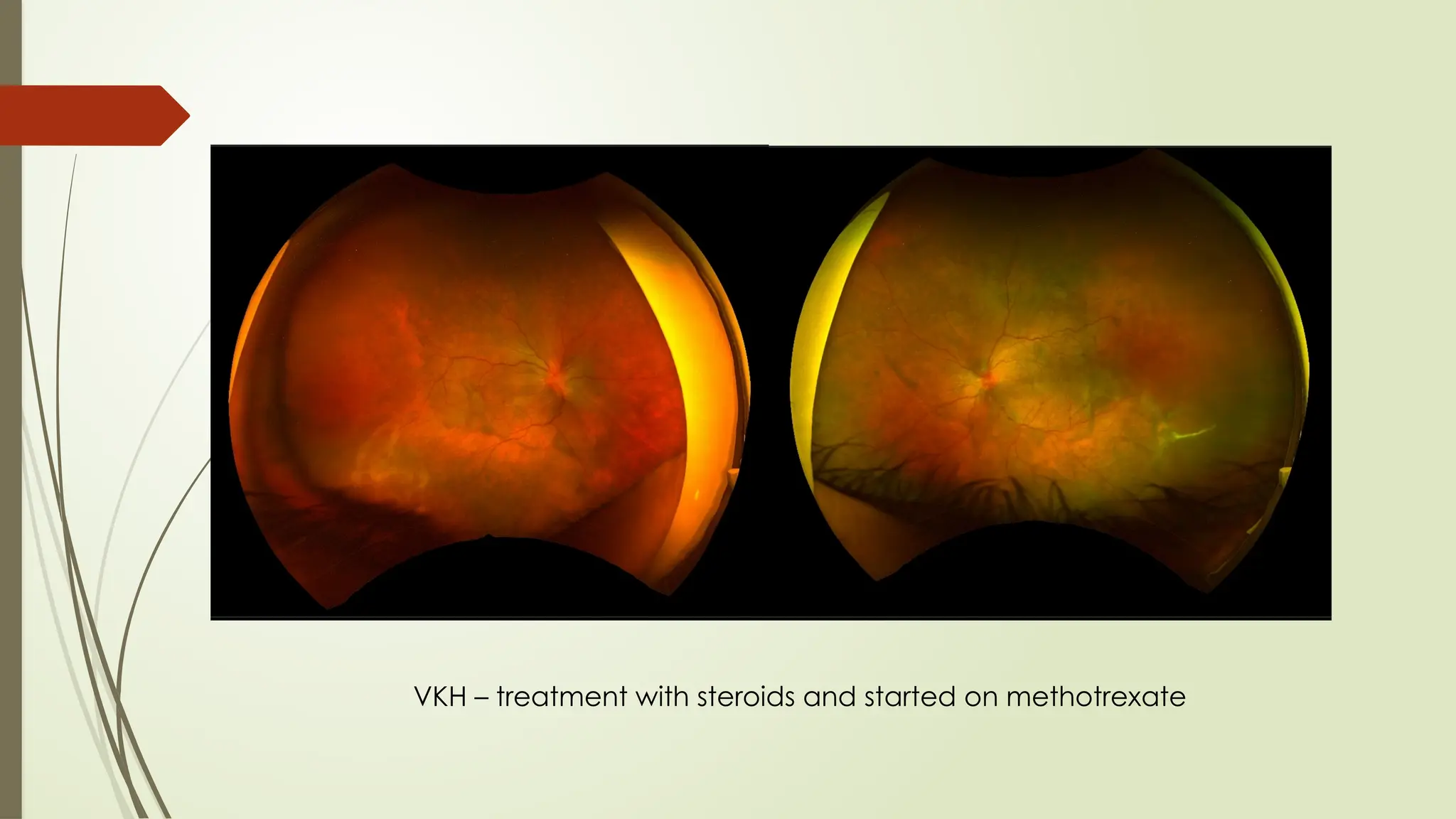
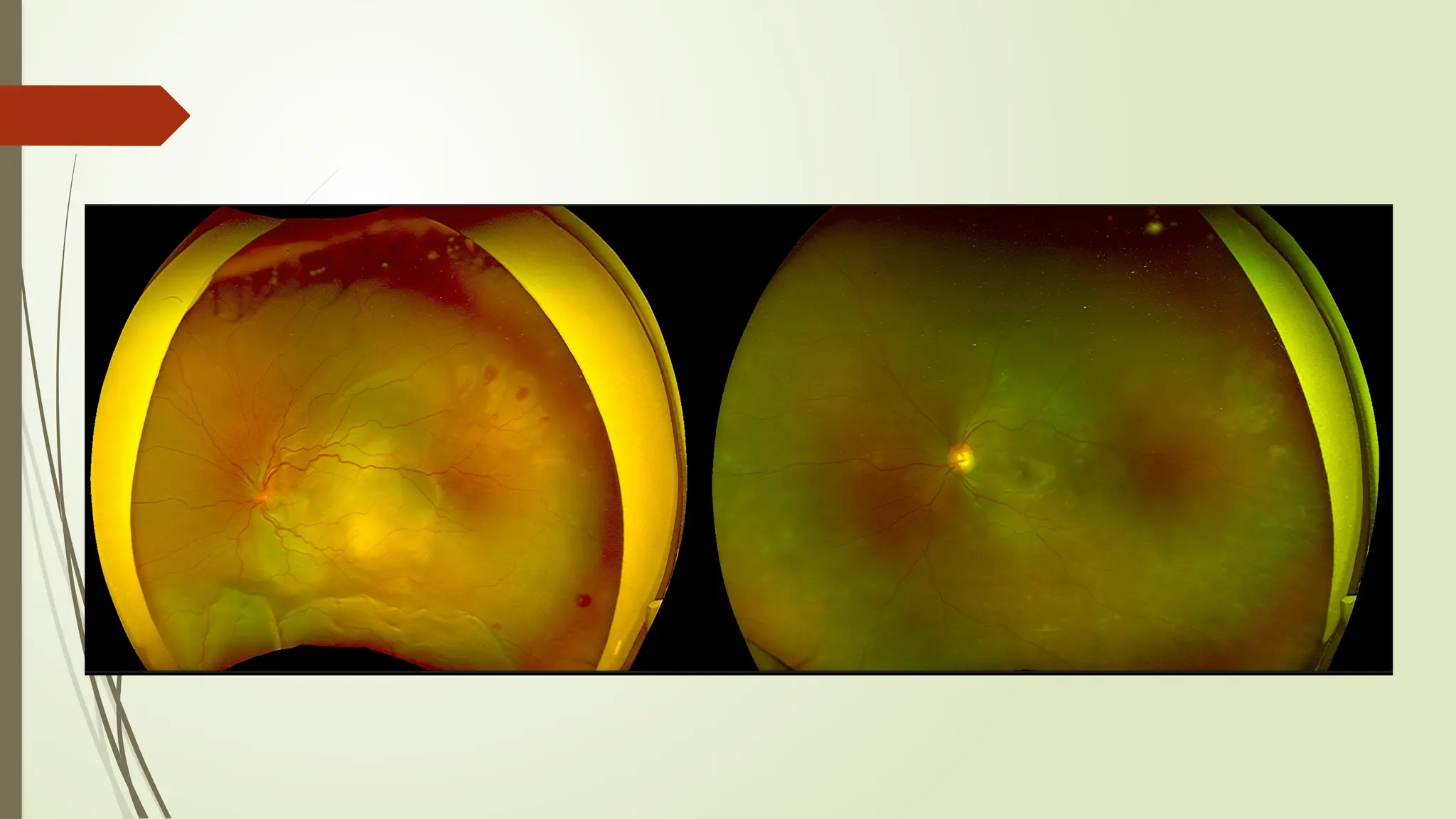
VKH Syndrome
Necrotizing sclerouveitis
Anti-Metabolites
Antimetabolites areoften the first immunomodulatory therapies used when corticosteroid
sparing is desired.
Azathioprine -
Purine analogue – prodrug of 6-mercaptopurine
Dose dependent, slow and persist after discontinuation
Dose start 1 mg/kg and then can be increased to 2.5 mg/kg
Effect start 2-4 weeks
slightly higher incidence of adverse effects
Complete blood counts and liver function tests must be closely monitored.
effective - Behcet disease, VKH, SO, Necrotizing uveitis
Myelosuppression, GIT upset, hepatotoxicity, hepatic veno-occlusive disease,
hypersensitivity pancreatitis
29.
Anti-Metabolites
Methotrexate
Folicacid antagonist – inhibit dihydrofolate reductase
10-25mg/week
PO, SC, IM
Effective – JIA associated anterior uveitis, sarcoidosis, panuveitis, and scleritis.
up to 6 months to produce its full effect in controlling intraocular inflammation
Gastrointestinal symptoms, hepatotoxicity, interstitial pneumonitis, pulmonary fibrosis
teratogenic, and complete blood counts and liver function tests (6-8 week) should be
conducted regularly.
30.
Anti-Metabolites
Mycophenolate mofetil
IMP dehydrogenase inhibitor (pyrimidine)
500 mg BD initially; max 1.5 mg
work rapidly - has a significantly shorter time to treatment success.
Costly
Less than 20% of patients have adverse effect; Diarrhoea, nausea, neutropenia
Regular laboratory monitoring required
Effective corticosteroid-sparing agent in up to 85% of patients with chronic uveitis.
Safe alternative to methotrexate in patients with pediatric uveitis.
31.
T-cell inhibitors
Cyclosporineand tacrolimus
fungus derivative - calcineurin inhibitors
Nephrotoxic, HTN, hyperkalemia, tremor, hirsuitism, gum hyperplasia
Patients with psoriasis - greater risk of primary skin cancers
Sirolimus
noncalcineurin inhibitor
inhibits antibody production and B lymphocytes
Effective – Behcet, posterior uveitis including VKH
32.
Alkylating agents
Cyclophosphamide,Chlorambucil
used only if other immunomodulators fail to control uveitis;
Considered for necrotizing scleritis associated with systemic vasculitides such as
granulomatosis with polyangiitis (formerly, Wegener granulomatosis) or relapsing
polychondritis.
Effective - Intermediate uveitis, VKH syndrome, sympathetic ophthalmia, and Behçet
disease.
BM suppression, hemorrhagic cystitis, malignancy, infection, infertility
high rate of sterility
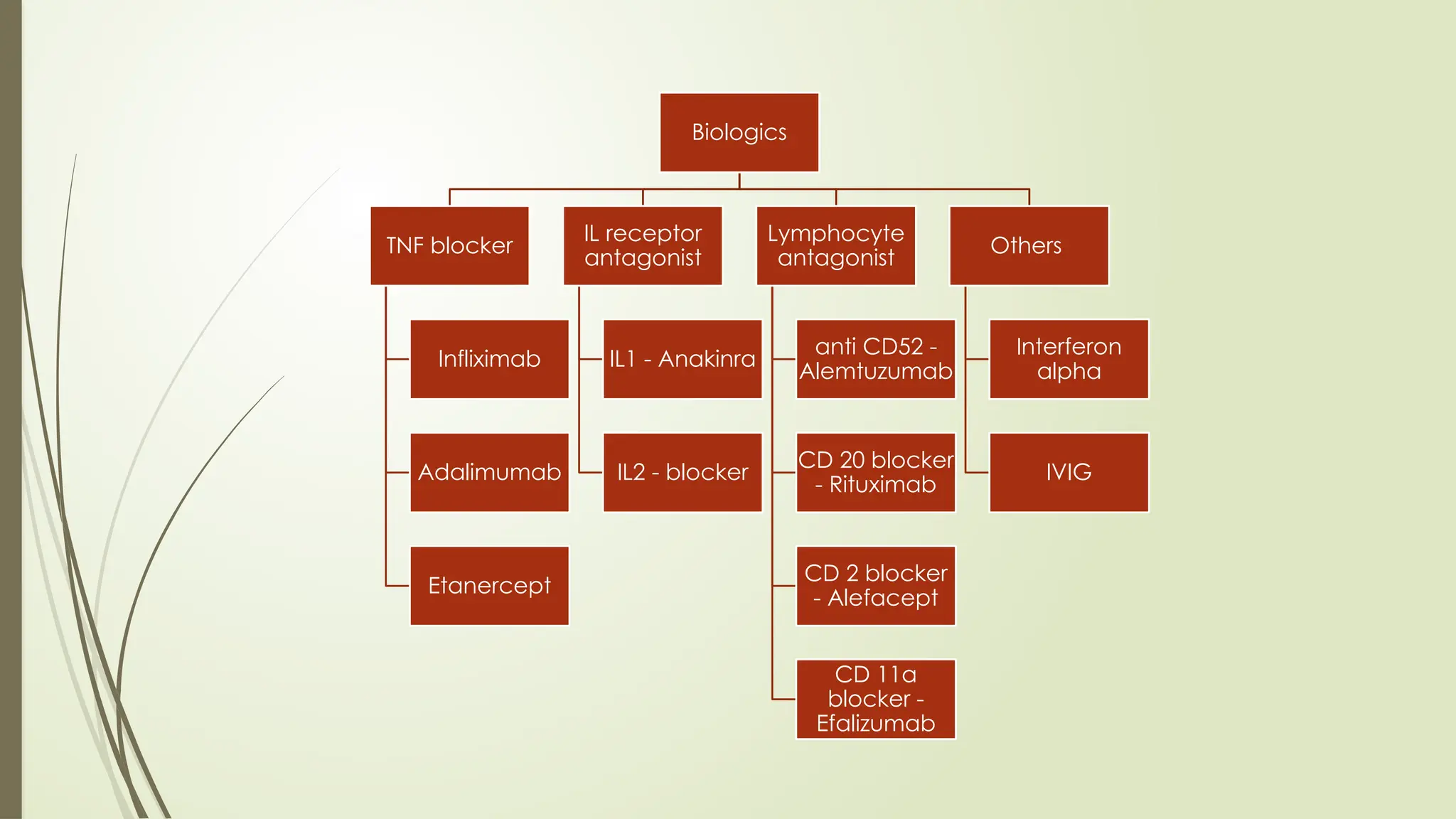
Adalimumab
NI Inetrmediate,posterior and panuveitis
40mg SC
Reduces risk of treatment failure in both active and non-active disease
VISUAL study
Nasopharyngitis, arthralgia, fatigue
#5 ROUTINE - Cbc esr dlc not of much help as they are non-specific and do not contribute much to the diagnosis
While they are imp in case of starting antimetabole for baseline and folllowup to detect bm suppression
In HIV cd4/cd8 ratio is imp
Suspicion of parasitic infection – raised esosinophils
#7 Active toxo; aids; cvd
RF – one must know it is seronegative arthritis like JRA and ankylosing spondylitis which are usually associated with uveitis compared to RF pos
Anterior uveitis in children get ANA titres as pauciarticular jra have iridocyc and 90% of these cases ANA associ
ANA – 99% SLE
Anti ds-dna; ANCA; ACE
Toxoplasmosis – strong clinical susp based on morphology……any positive titre with strong clinical susp indicate treatment while neg excludes the diag but if healed not of much use of such test
Ant seg exam
S ace level monitor disease activity and response ; pos 85% cases active
X ray; sacroiliac joint; skull( calcific in cong toxo)
Hla b27; b5; a29
Skin - tb histoplasmosis, anergy in sarcoidosis
Histoplasmin test -
POHS, may reactivate older lesions.
Kveim test
Sarcoidosis, No longer used
#8 RF – one must know it is seronegative arthritis like JRA and ankylosing spondylitis which are usually associated with uveitis compared to RF pos
ANA titres must be done as 90% of these cases are
Histoplasmin test -
POHS, may reactivate older lesions.
Kveim test
Sarcoidosis, No longer used
#10 The goal of medical management of uveitis is to effectively control inflammation so as to eliminate or reduce the risk of vision loss from structural and functional complications that result from uncontrolled inflammation—cataracts, glaucoma, CME, and hypotony
#11 The goal of medical management of uveitis is to effectively control inflammation so as to eliminate or reduce the risk of vision loss from structural and functional complications that result from uncontrolled inflammation—cataracts, glaucoma, CME, and hypotony
#14 Greter the severity of inflamm; greater threat to vision; more intense and rapid resolution
#15 GC pass through cytoplasmic membrane to bind to the cytosolic glucocorticoid receptor (cGCR), displacing several associated proteins (heat shock proteins hsp, kinases like mitogen activated protein kinase/MAPK and co-chaperones like src) that mediate nongenomic effects. The GC-cGCR complex moves into the nucleus to affect transcription by ways depicted above. (i) and (ii) involve binding of cGCR to positive and negative glucocorticoid responsive elements (GRE and nGRE); in (iii) binding of cGCR is prevented by competition for nuclear coactivators between the cGCR and transcription factors like activator protein 1 (AP1); (iv) involves transrepression due to direct or indirect interaction of the cGCR with transcription factors such as nuclear factor-kB (NF-kB) at its binding site (kB site). Non-genomic effects are also suggested to be mediated through membrane bound GCR (mGCR) and by interactions with cellular membranes.
#16 Response to treatment - improvement/ stabilization of va; media clarity; cells ; decrease in symptoms; regression of lesion
Steroid resist – when no clinical resp on 2 weeks of max dosage of oral steroids
#17 Retisert – 2.5 years 0.59 mg high rates of glaucoma and cataract
#18 Retisert – 2.5 years 0.59 mg high rates of glaucoma and cataract
#28 Primary immunological abnormality leading to inflamm
Immunosprresive act on all immune cells non-specifically
Thus suppress activity of normal cells as well
Thus importance of risk benefit ratio
#29 The use of IMT in uveitis is warranted for consideration in the following settings:
vision-threatening intraocular inflammation
disease process that is likely reversible
corticosteroids contraindicated because of systemic problems or intolerable adverse effects
unacceptable corticosteroid adverse effects
long-term corticosteroid dependence
these drugs should also be considered in patients who require long-term
corticosteroid therapy (longer than 3 months) at doses greater than 5–10 mg/day.
#33 Many clinicians start administering azathioprine at 50 mg/day for 1 week to watch for
development of any gastrointestinal adverse effects (nausea, upset stomach, and vomiting) before
escalating the dose. These symptoms are common and may occur in up to 25% of patients,
necessitating discontinuation.
Bone marrow suppression is unusual at the doses of azathioprine used
to treat uveitis. However, patients taking allopurinol and azathioprine concomitantly are at higher risk
for bone marrow suppression. Reversible hepatic toxicity occurs in less than 2% of patients, and
dose reduction may remedy mild hepatotoxicity.
MYELOSUPPRESION – early (idiosyncratic) and delayed response (dose- dependent)… weekly * 1m twice a month for 3 m then monthly
#34 Affect humoral immunity mainly and minim on CMI. Also releases adenosine which has anti-inflammatory actions
Any pt with cough dyspnea - get a chest x ray to rule out interstitial pneumonitis
#35 Many clinicians start administering azathioprine at 50 mg/day for 1 week to watch for
development of any gastrointestinal adverse effects (nausea, upset stomach, and vomiting) before
escalating the dose. These symptoms are common and may occur in up to 25% of patients,
necessitating discontinuation.
Bone marrow suppression is unusual at the doses of azathioprine used
to treat uveitis. However, patients taking allopurinol and azathioprine concomitantly are at higher risk
for bone marrow suppression. Reversible hepatic toxicity occurs in less than 2% of patients, and
dose reduction may remedy mild hepatotoxicity.
#36 that eliminate T-cell receptor signal transduction and downregulate interleukin-2 (IL-2) gene transcription and receptor expression of CD4+ T lymphocytes.
#37 The most worrisome adverse effect of alkylating agents is an increased risk of malignancy
Cyclophosphamide
Lymphotoxicity
Chlorambucil Dna crosslinking
Patients with polycythemia rubra vera - chlorambucil - 13.5-fold greater risk of leukemia. Patients with granulomatosis with polyangiitis - cyclophosphamide - 2.4-fold increased risk of cancer and a 33-fold increased risk of bladder cancer
#39 recombinant human
immunoglobulin G1 monoclonal antibody that binds
specifically to TNF-a (a proinflammatory cytokine produced
predominantly by macrophages and T cells
inhibits (with a half-maximal inhibitory concentration of
0.1–0.2 nmol/L) the adhesion molecules responsible for
leukocyte migration (endothelial-leukocyte adhesion
molecule-1, intracellular adhesion molecule-1 and vascular
cell adhesion molecule-1)
therapy with adalimumab was associated with significant
reductions in plasma vascular endothelial growth factor
(VEGF) levels
Two double-blind, placebo-controlled, multinational, phase
III studies evaluated the therapeutic efficacy of subcutaneous
adalimumab in adults (aged C18 years) with active
(VISUAL I [11]) or inactive (VISUAL II [12]) non-infectious,
intermediate, posterior or panuveitis (Sect. 4.1).
Patients with isolated anterior uveitis were excluded
[11, 12]. Longer-term efficacy data (derived from an
abstract [13]) from an open-label extension of these studies
(VISUAL III), which was primarily designed to evaluate
the safety and tolerability of adalimumab, are also
reviewed