ROLE OF ANURSE IN
PREVENTIVE PSYCHIATRY
PRESENTED BY: Miss. Sharley Masih
2.
OBJECTIVES:
Introduction to preventivepsychiatry.
Describe the levels of prevention.
Explain the role of nurse in primary, secondary and tertiary
prevention
Define rehabilitation
Enlist the principles of rehabilitation
Discuss psychiatric rehabilitation approaches
3.
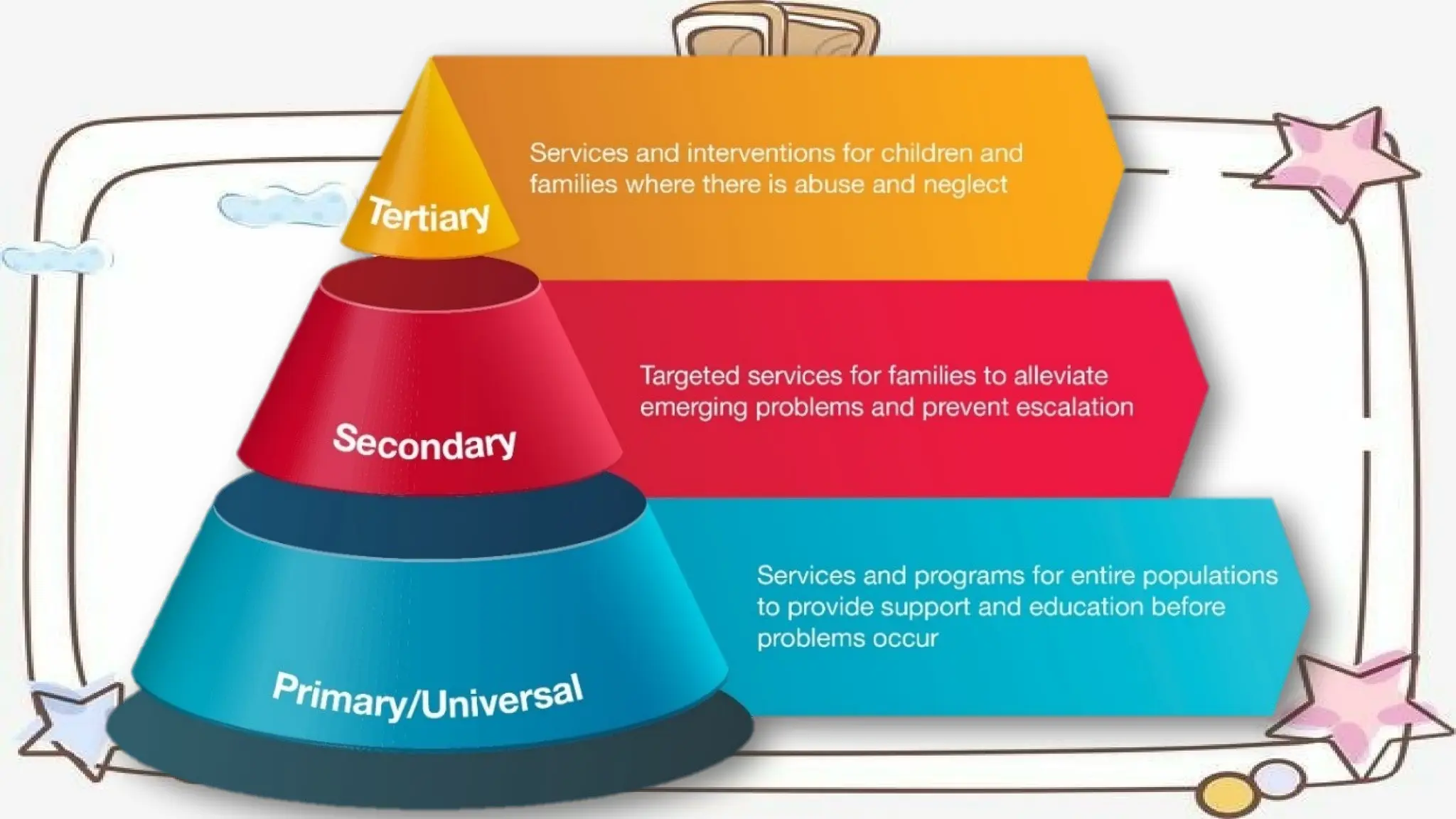
LEVELS OF
PREVENTION
In 1964Psychiatrist GERALD CAPLAN describe levels of prevention specific
to psychiatry.
He described primary prevention as an efforts direct towards reducing in
incidence of mental disorder in a community.
Secondary prevention refers to decreasing the duration of disorder while,
tertiary prevention refers to reducing the level of impairment.
INTRODUCTION
Primary prevention seeksto prevent the occurrence of
mental disorders by strengthening individual, family and
group coping abilities
Primary prevention
7.
• AIM :Reducing the incidence of mental disorder within the population.
• TARGET: Individual, Environment.
• STRATERGIES: Assisting individual to increase their ability to cope effectively
with stress. Targeting and diminishing harmful forces i.e., stressor within the
environment.
8.
ROLE OF ANURSE
1. INDIVIDUAL CENTERED INTERVENTION
Antenatal care to the mother and educating her regarding the
adverse effects of irradiation, certain drugs and prematurity
Dietary corrections to those infants suffering from metabolic
disorders.
Correction of endocrine disorders.
Liberalization of laws regarding termination of pregnancy, when it
is unwanted.
9.
Counselling theparents of physically and mentally handicapped
children, with particular reference to the nature of defects.
Fostering bonding behaviors.
Explaining importance of warm, accepting, intimate relationship and
avoiding the prolonged separation of mother and child are
essential.
10.
2. INTERVENTIONS ORIENTEDTO THE CHILD IN THE SCHOOL
Teaching growth and development to the parents and teachers.
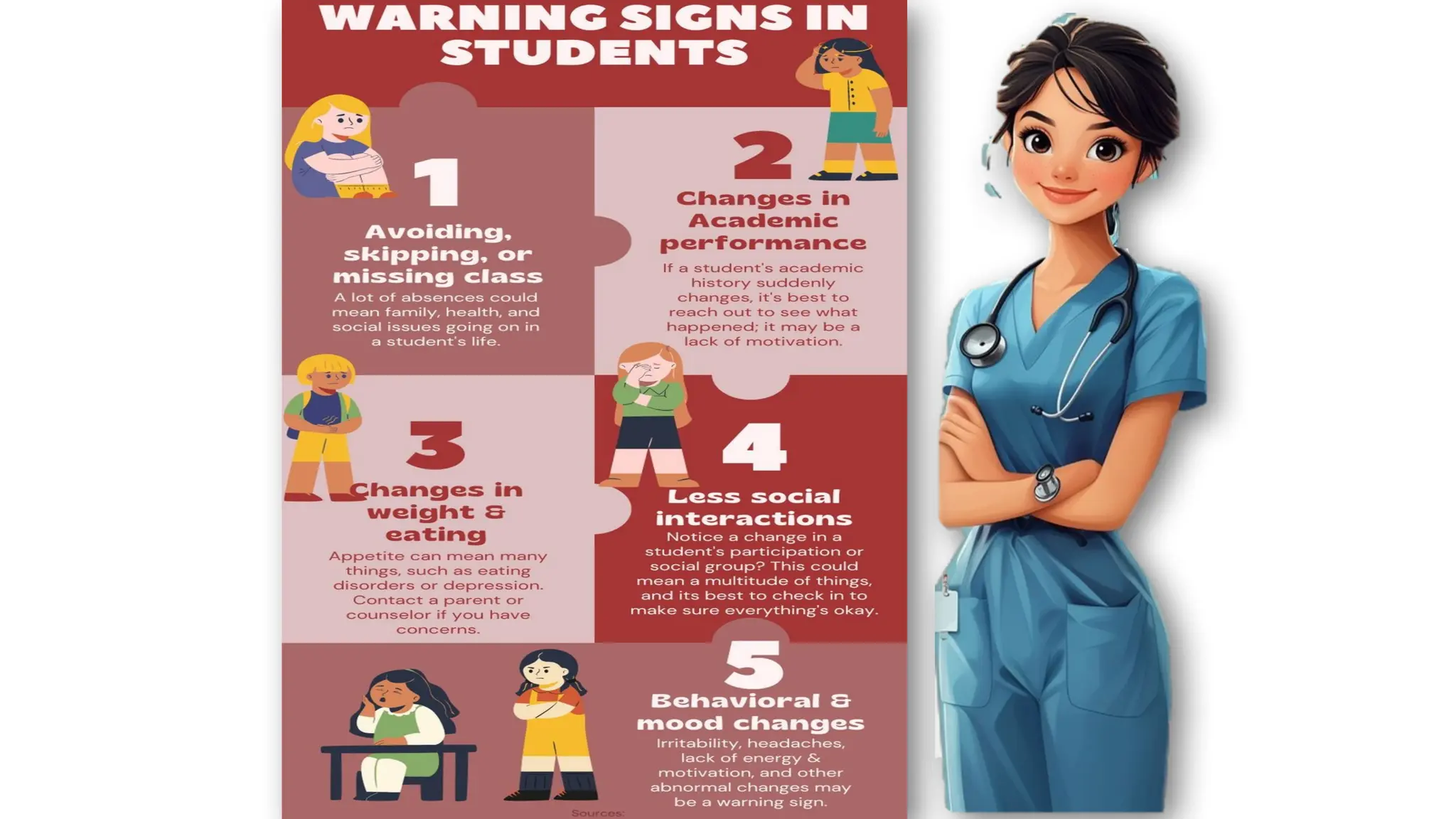
Identifying the problems of scholastic performance and emotional
disturbances among school children.
School teachers can be taught to recognize the beginning symptoms of
problems and referring to appropriate agencies
12.
3.FAMILY CENTERED INTERVENTIONSTO ENSURE HARMONIOUS
RELATIONSHIP
Consulting with parents about appropriate disciplinary measures.
Promoting open health communication in families.
Rendering crisis counselling to the parents of physically and mentally
handicapped children.
Ensuring harmonious relationship among members of the family and
teaching healthy adaptive techniques at the time of stress producing
events
13.
4.INTERVENTION ORIENTED TOKEEP FAMILIES INTACT
Mental health education about child rearing practices.
Strengthening for the social support for the frustrated aged and helping
them to retain their usefulness.
Promoting educational services in the field of mental health and
mental hygiene.
Providing marital counselling for those having marital problems.
14.
5. INTERVENTION FORFAMILIES IN CRISES
In developmental crisis situations such as the child passing
through adolescence, birth of new baby, retirement or
menopause, death of wage earner by the family describe by
the spouse etc.
Crisis intervention can be given at :-
Mental hygiene clinics
Psychiatric first-aid centers
Walk-in clinics
15.
6.MENTAL HEALTH EDUCATION
Conduct mass health education programs through film shows, flash
cards and appropriate audio-visual aids regarding prevention of
mental illness and promotion of mental health in the community.
Educate health workers regarding prevention of mental illness.
16.
7. SOCIETY-CENTERED PREVENTIVEMEASURES
Community development culturally deprived families need
biological and psychosocial supplies.
They need better hygienic living conditions, proper food,
education, health facilities and recreational facilities.
Otherwise, psychopathy, alcoholism, crime and mental illness, will
result in such situations.
Collection and evaluation of epidemiological, biostatical data.
17.
Secondary Prevention
Secondary preventiontargets people who show early symptoms
of mental health disruption but regain premorbid level of
functioning through aggressive treatment.
18.
TARGET:
• Recognition ofsymptoms and provision of referral for treatment.
• Ongoing assessment of individuals at high risk for illness
During home visit.
Day care or community health center.
19.
ROLE OF ANURSE
1.EARLY DIAGNOSIS AND CASE FINDING
This can be achieved by educating the public community
leaders in how to recognize early symptoms of mental illness.
Community mental health nurse detect:
Early signs of increased levels of anxiety, decreased ability to
cope with stress and provide direct services as appropriate.
20.
2. EARLY REFRRENCE
Thepublic should be educated to refer these cases to proper hospitals as
soon as they recognize early symptoms of mental illness.
3.TRAINING OF HELATH PERSONNEL
Orientation courses, should be provided to health workers to detect
cases in the course of their routine work.
21.
4. SCREENING PROGRAMS
Simple questionnaires should be developed to identify the
symptoms of mental illness in the community.
Early and effective treatment for patient, and family members,
provide counselling services to caregivers of mentally ill patients.
22.
5. CONSULTATION SERVICES
Nurses working in general hospitals may come across various
conditions such as puerperal psychosis, anxiety states, peptic ulcers,
ulcerative colitis, bronchial asthma etc.
These basic care provides need guidance and consultation to deal with
these conditions in an effective manner.
6. CRISIS INTERVENTION
If crises is not tackled in time it may lead to suicide or mental disorder.
23.
Tertiary prevention
Tertiary preventiontargets those with mental illness and help to
reduce the severity, discomfort and disability associated with
their illness.
24.
AIM: Reducing theresidual defects that are associated with severe
and persistent mental illness.
STRATERGIES:
• Preventing complications of the illness.
• Promoting rehabilitation that is directed towards the achievement of
each individuals maximum levels of functioning
25.
Disability
Disability is “anyrestriction or lack of ability to perform an
activity in the manner or within the range considered normal
for the human being”.
26.
ROLE OF ANURSE
Family involvement
Occupational and recreational activities
Rehabilitation
Teaching the client daily living skills
Encouraging independence
Referring clients to various aftercare services
Community based programmes
27.
PSYCHIATRIC REHABILITATION
Rehabilitation isthe process of enabling the individual to return his highest
possible level of functioning.
It is an important component of the community mental health program, and is
under taken at the level of tertiary prevention.
28.
REHABILITATION
Rehabilitation is “anattempt to provide the best possible community
role which will enable the patient to achieve the maximum range of
activity, interest and of which he is capable”.
-Maxwell Jones (1952)
Indications
The following disordersare indicated commonly for rehabilitation:-
Chronic schizophrenia
Chronic organic mental disorders
Mental retardation
Alcohol and drug dependence
31.
Increasing independencewould be the first step in
rehabilitation process.
Primary focus is on improvement of abilities and
competence of clients with psychiatric problems.
Maximum use must be made of residual capacities.
Patient's active participation is very essential.
Skill development therapeutic environment are
fundamental interventions for a successful rehabilitation
process.
PRINCIPLES OF REHABILITATION
PSYCHIATRIC REHABILITAION APPROACHES
Psycho education: Includes diagnosing the problem, telling the person
what to expect regarding illness and discussing treatment alternatives.
Working with families: Encouraging family members to get involved in
treatment and rehabilitation programs.
34.
Group therapy:Positive aspects of group therapy include and
opportunity for ongoing contact with others, sharing their views about
problem solving abilities.
Social skills training: It involves teaching specific living skills that the
patient is expected to have in order to survive in the community.















![21549552 Psychiatric Nursing[1]](https://cdn.slidesharecdn.com/ss_thumbnails/21549552-psychiatric-nursing1-100616064539-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


































