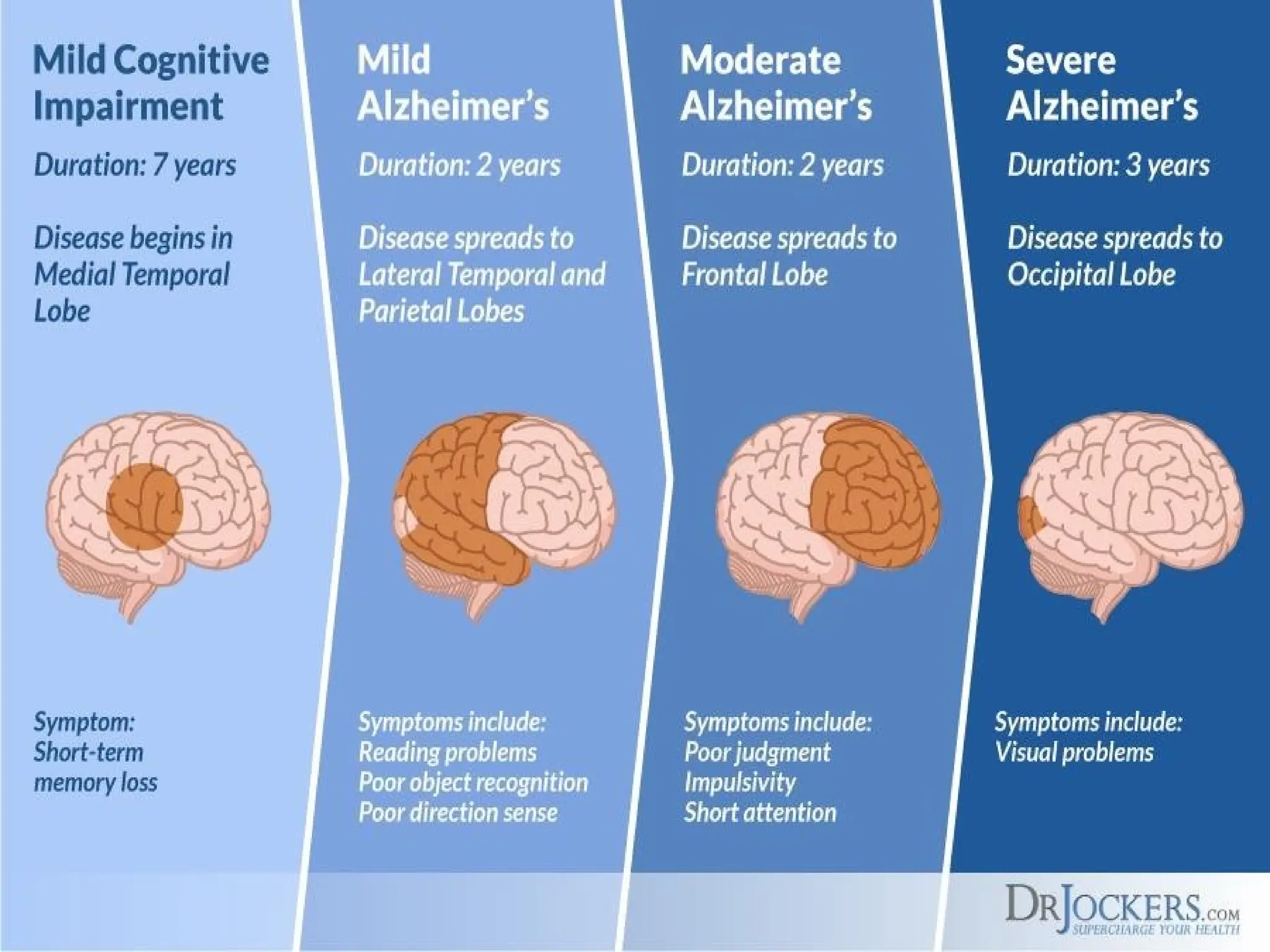
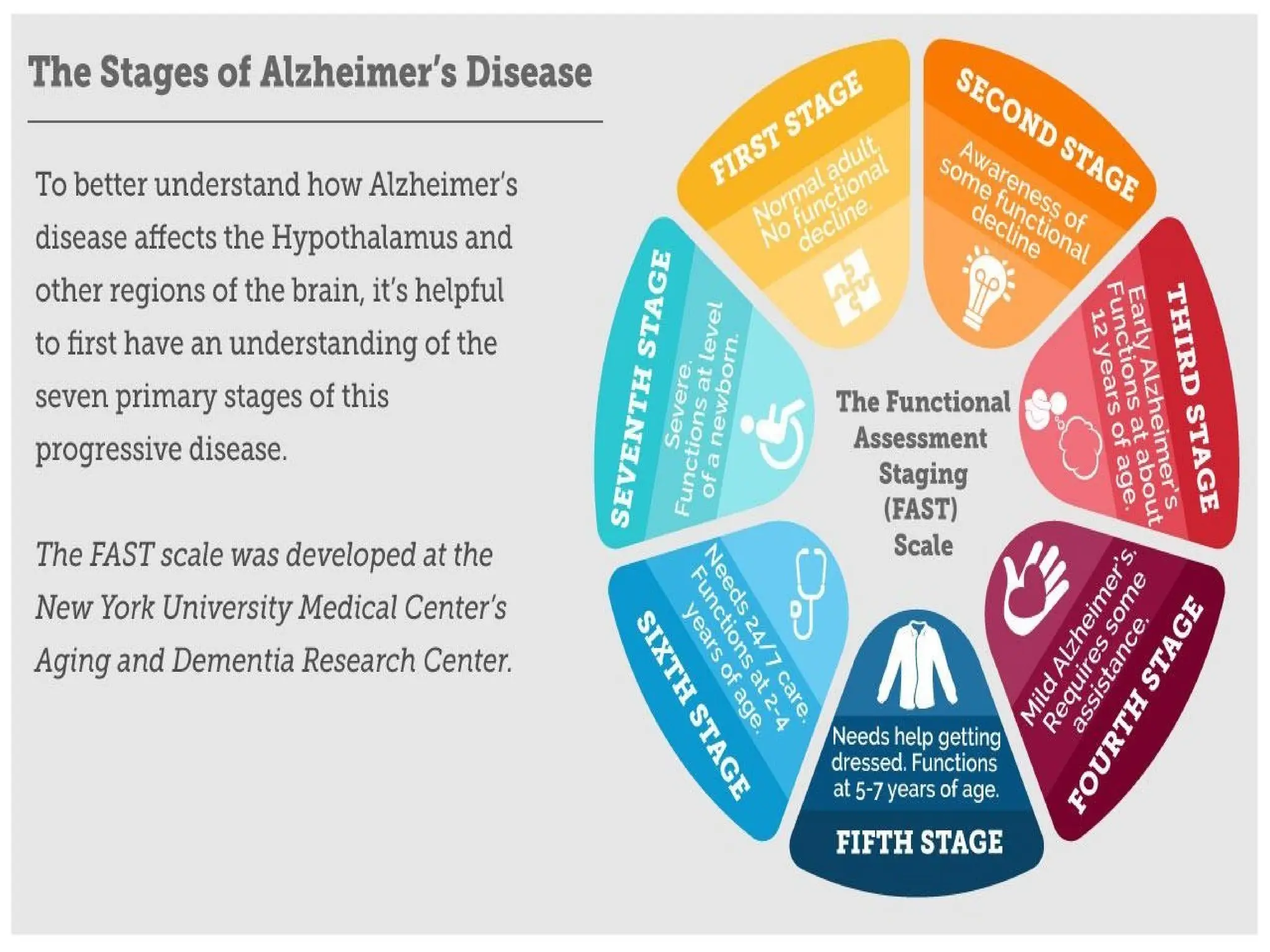
Alzheimer’s disease isan irreversible, progressive brain
disease that slowly destroys memory and disorders
cognitive function
6.
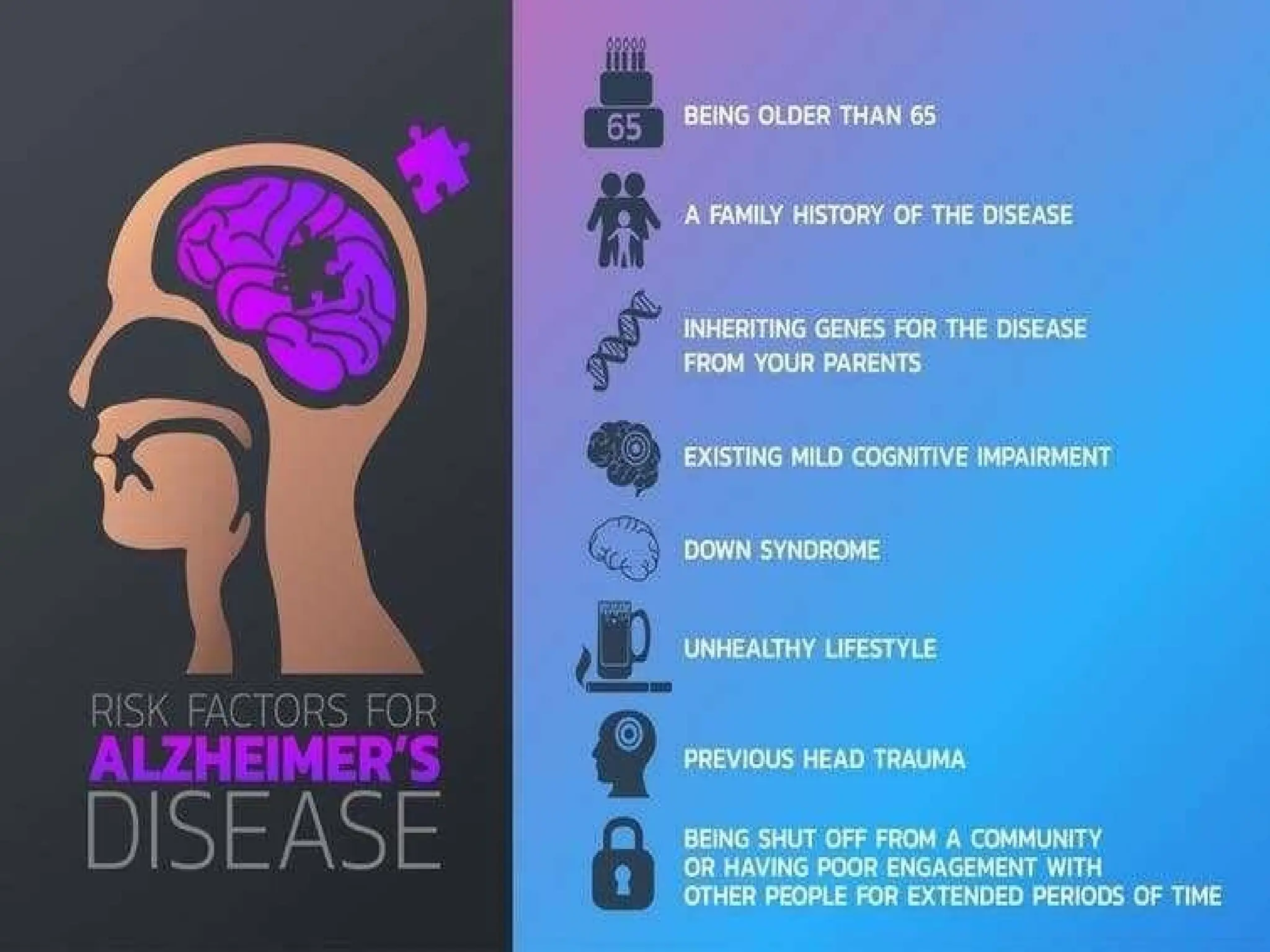
Although the riskof developing AD increases with age – in
most people with AD, symptoms first appear after age 60
(5% incidence) AD is not a part of normal aging.
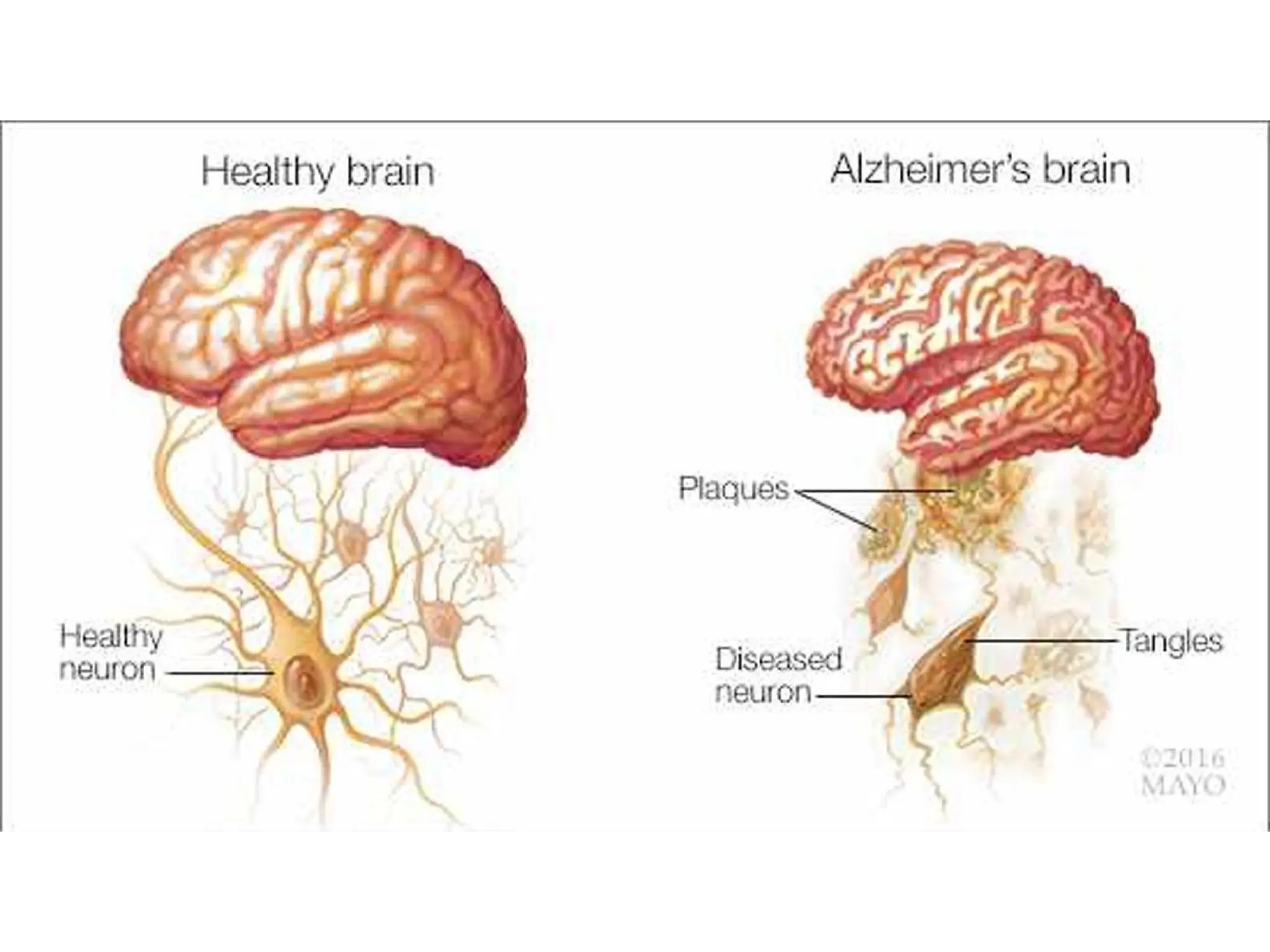
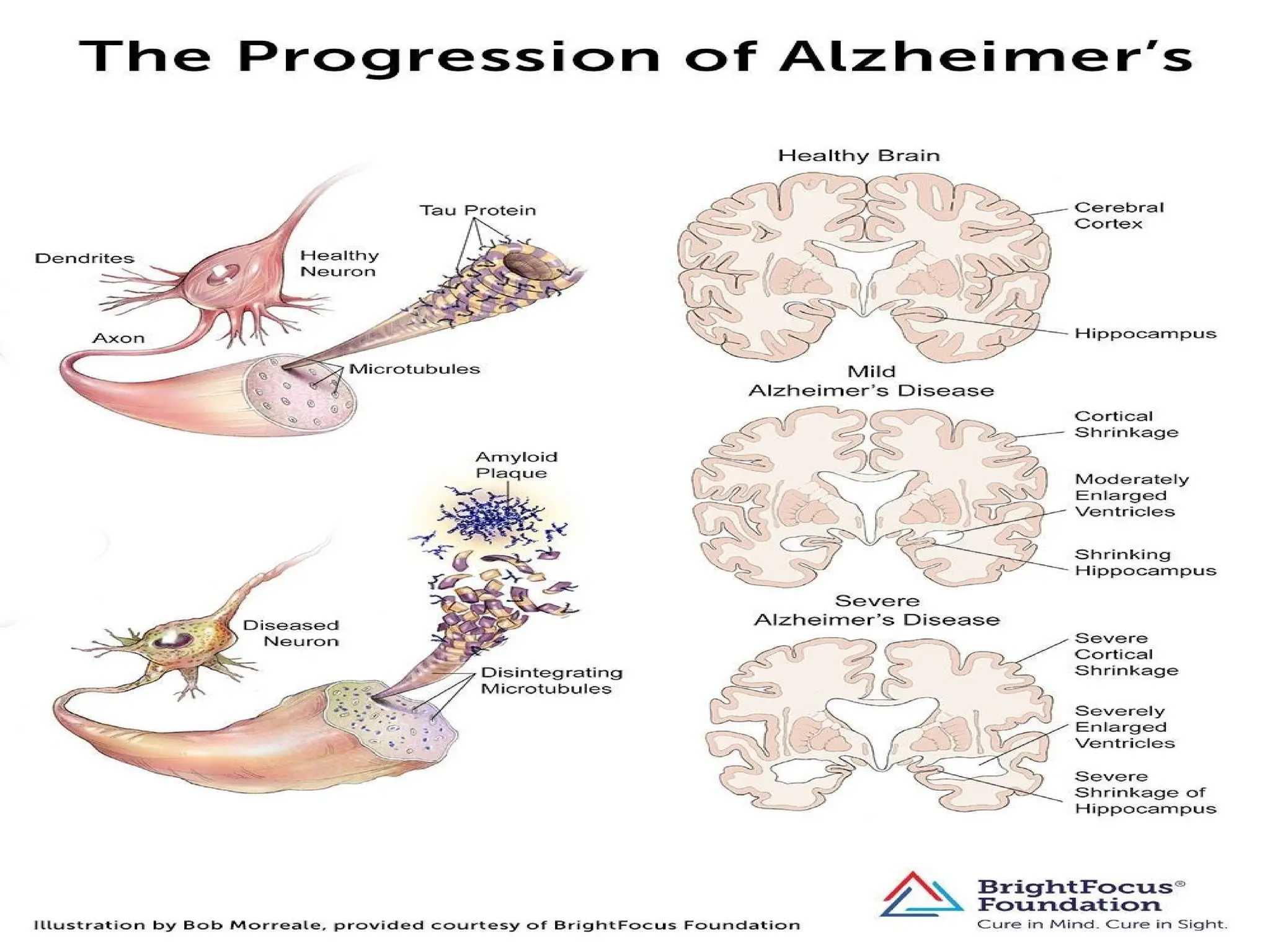
Microscopically:
– Changes inthe proteins of the nerve cells of the
cerebral cortex
– accumulation of neurofibrillary tangles and
neuritic plaques (deposits of protein and altered
cell structures on the interneuronal junctions)
granulovascular degeneration
– loss of cholinergic nerve cells (important in
memory, function, cognition
Diagnosis
• Medical history,history from relatives, and
behavioural observations.
• Neurological Examination and MSE
• CT, MRI, SPECT, PET can be used to help
exclude other cerebral pathology
21.
Lab diagnosis
• completeblood count, sedimentation rate,
chemistry panel, thyroid-stimulating
hormone, test for syphilis, urinalysis, serum
B12, folate level, and test for HIV
• to rule out infectious or metabolic
disorders
22.
• cerebrospinal fluid(CSF) - tau protein and
beta-amyloid
Genetic testing
In families with a history of Alzheimer's
disease, test to confirm AD or to provide
information to at-risk family members regarding
their likelihood for development of AD
23.
How is Alzheimer’sDisease managed at present?
• Ideally, management should involve an interdisciplinary
approach for assessment, treatment & education
• The roles of nutritionists, caregivers, nurses, social workers
and patients associations can be vital for the long term care
• Pharmacological treatment
– Cholinesterase inhibitors
– Memantine
24.
The 3 targetsfor Pharmacotherapy
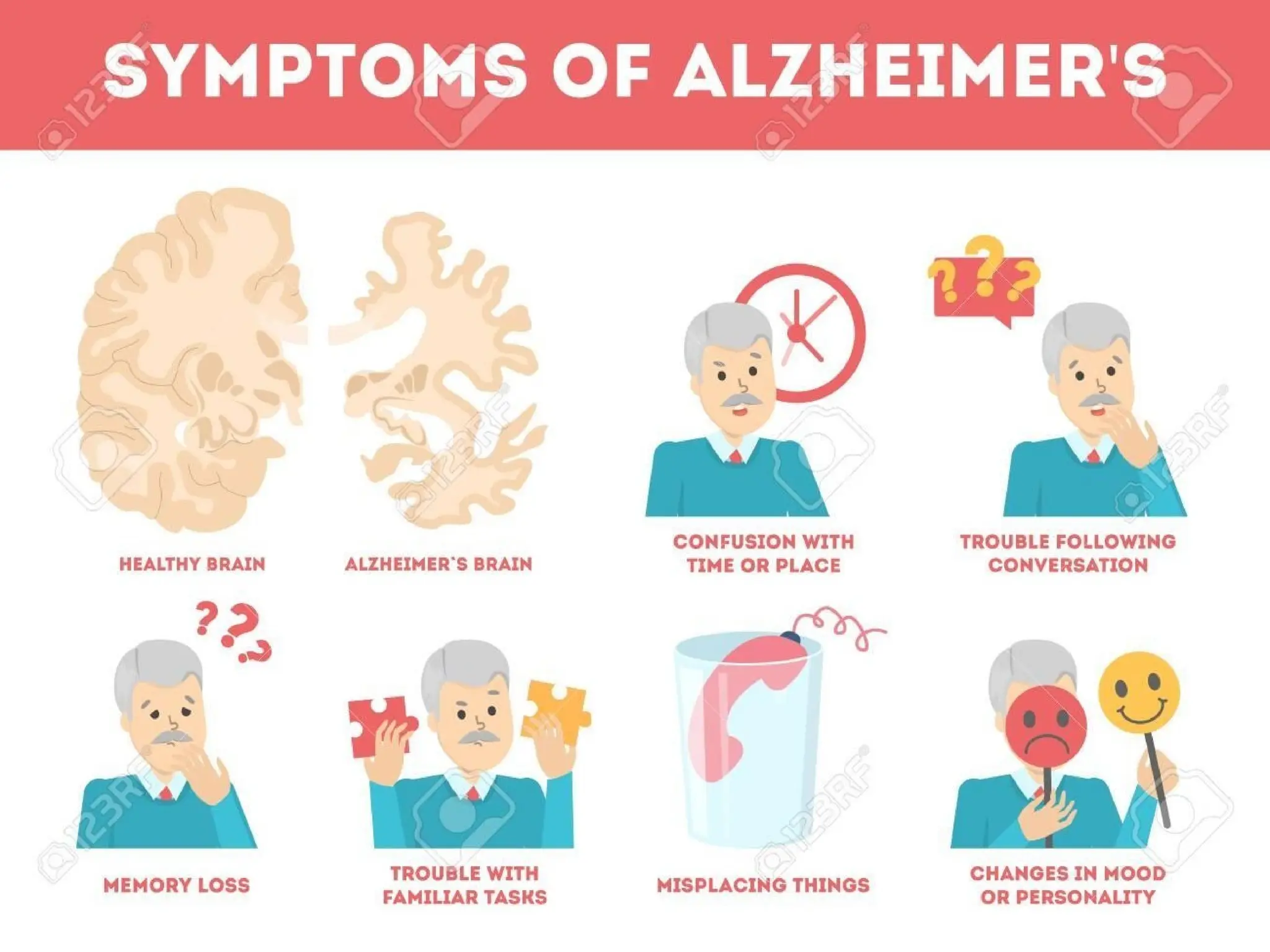
•Cognitive decline: memory, language,
orientation, concentration, etc.
•Behavioral abnormalities: delusions,
aggressiveness, anxiety, depression, psychosis
etc..
•Activities of Daily Living: dressing, bathing,
feeding, use of household appliances, etc
Nicotine is acholinergic agonist that acts both
postsynaptically and pre-synaptically to release
acetylcholine
Melatonin - This neurohormone prevents
neuronal death caused by exposure to the
amyloid beta protein
27.
Donepezil (Aricept)
• Widelyused in mild to moderate cases
because it can be given once daily and is well
tolerated
• Starting at 5 mg hs and increased to 10 mg
after 4 to 6 weeks
28.
Galantamine
• Given withfood in dosage of 4 to 12 mg bid
Should be restarted at 4 mg bid if interrupted
for several days
• Dose should be reduced in cases of renal or
hepatic impairment
Memantine
• NMDA-receptor antagonist
•The first of a new class approved for moderate
to severe Alzheimer's
• Dosage is 10 mg bid
• Can be used with a cholinesterase inhibitor
31.
• Patients withdepressive symptoms should be
considered for antidepressant therapy
• Behavioral disturbances may require
pharmacologic treatment anxiolytics,
antipsychotics, anticonvulsants
32.
Nonpharmacologic treatments usedto improve
cognition:
• Environmental manipulation that decreases
stimulation
• Aromatherapy, Massage, Music therapy,
Exercise
33.
Drug Alert
• Cholinesteraseinhibitors initially aimed at improving memory and
cognition seem to have an important impact on the behavioral
changes that occur in patients with cognitive impairment
• improves the apathy, disinhibition, pacing, and hallucinations
commonly noted in dementia
• Be alert for drug interactions with NSAIDs, succinylcholine-type
muscle relaxants, cholinergic and anticholinergic agents, drugs that
slow the heart, and other drugs
34.
Nursing assessment
• Performcognitive assessment
• Orientation, insight,
abstract memory, verbal ability
thinking, concentration,
• Assess for changes in behavior and ability to perform adls
• Evaluate nutrition and hydration
• Check weight, skin turgor, meal habits
• Assess motor ability, strength, muscle tone, flexibility
35.
Nursing diagnoses
• Self-caredeficit
• Constipation
• Disabled family coping
• Disturbed thought
• Imbalanced nutrition: Less than body
requirements Impaired verbal communication
36.
• Ineffective coping
•Interrupted family processes
• Risk for infection
• Risk for injury
37.
Intervention
s
• Establish aneffective communication system
with the patient and his family to help them
adjust to the patient's altered cognitive
abilities
• Provide emotional support to the patient and
his family
• Encourage them to talk about their concerns
• Listen carefully to them
38.
• Use asoft tone and a slow, calm manner when
speaking to him Because the patient may
misperceive his environment
• Allow the patient sufficient time to answer
your questions his thought processes are slow,
impairing his ability to communicate verbally
39.
Interventio
n
• Administer orderedmedications to the patient
and note their effects
• If the patient has trouble swallowing, check with
a pharmacist to see if tablets can be crushed or
capsules can be opened and mixed with a semi-
soft food
• Protect the patient from injury
• Provide a safe, structured environment
• Provide rest periods between activities because
these patients tire easily
40.
• Encourage thepatient to exercise to help
maintain mobility
• Encourage patient independence allow ample
time for the patient to perform tasks
• Encourage sufficient fluid intake and adequate
nutrition Provide assistance with menu selection
allow the patient to feed himself as much as he
can
• Provide a well-balanced diet with adequate fiber
• Avoid stimulants, such as coffee, tea, cola, and
chocolate
41.
• Give thepatient semisolid foods if he has dysphagia
• Insert and care for a nasogastric tube or a gastrostomy
tube for feeding as ordered
• Because the patient may be disoriented or
neuromuscular functioning may be impaired, take the
patient to the bathroom at least every 2 hours
• Assist the patient with hygiene and dressing as
necessary
• Many patients with Alzheimer's disease are incapable
of performing these tasks
Preventio
n
It is nota preventable condition.
Lifestyle risk factors for Alzheimer's can be
modified.
Changes in diet, exercise and habits — steps to
reduce the risk of cardiovascular disease — may
also lower your risk of developing Alzheimer's
disease
44.
Heart-healthy lifestyle choicesthat may reduce
the risk of Alzheimer's include the following:
• Exercise regularly
• Eat a diet of fresh produce, healthy oils and
foods low in saturated fat
• Follow treatment guidelines to manage high
blood pressure, diabetes and high cholesterol
• Quit smoking