Cardiogenic shock occurswhen the heart has
been damaged so much, that it is unable to
supply enough blood to the vital organs of the
body. As a result of the failure of the heart to
pump enough nutrients to the body, blood
pressure falls and organs may begin to fail.
Cardiogenic shock is uncommon, but when it
does occur, it’s a serious medical emergency.
INTRODUCTION
2.
Cardiogenic shock isthe failure of heart to
pump blood adequately to meet the
oxygenation needs of body. ( Cardiovascular
Medicine)
Cardiogenic Shock is defined as the hearts
inability to contract and pump the blood
effectively due to inadequate supply of
oxygen and nutrients to the body.
DEFINITION
3.
Incidence rateof cardiogenic shock is
43.7%.
40 to 70 % cardiogenic shock is with
Acute MI
INCIDENCE
Classification basedon .
Coronary cardiogenic shock
Non coronary Cardiogenic shock
CORONARY CARDIOGENIC SHOCK
Coronary cardiogenic shock occurs when the
significant amount of the left ventricular
myocardium has been damaged.
Eg Myocardial infraction.
More common
.
6.
NON CORONARYCARDIOGENIC
SHOCK
Occur mainly due to stress to myocardium.
Examples severe hypoxemia
Acidosis
Hypoglycaemia
Tension pneumothorax
.
.
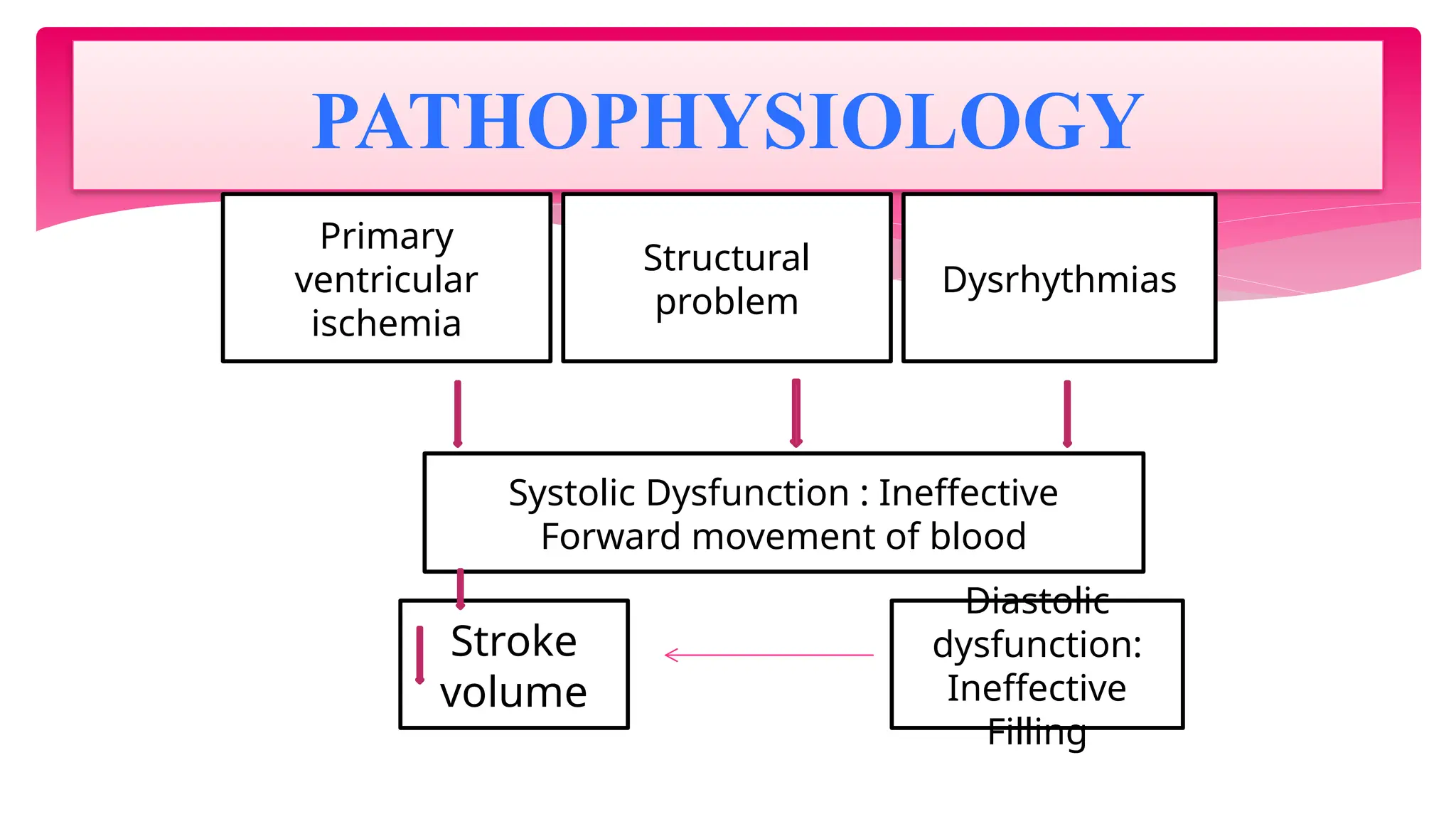
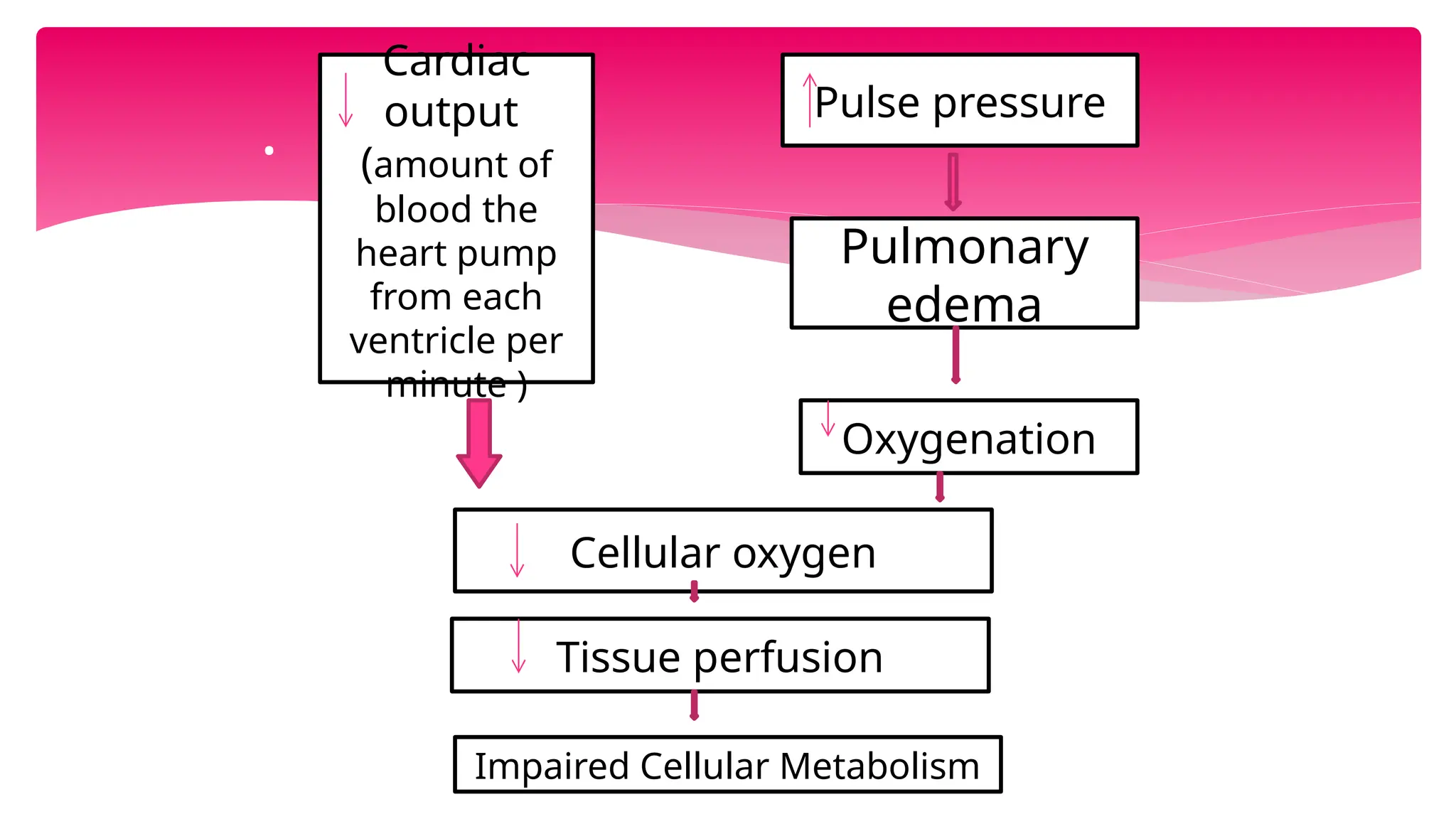
Cardiac
output
(amount of
blood the
heartpump
from each
ventricle per
minute )
Pulse pressure
Pulmonary
edema
Oxygenation
Cellular oxygen
Tissue perfusion
Impaired Cellular Metabolism
10.
1. The classicsigns and symptoms of cardiogenic
shock are the heart muscle loses it’s contractle
power, resulting in a marked reduction of SV and CO.
2. Confusion, restlessness, mental lethargy ( due to
poor perfusion of brain)
3. Low Systolic Blood pressure
4. Oliguria ( urine output less than 30ml/hr( due to
decrease perfusion of kidneys)
5. Chest pain( due to lack of oxygen and blood to heart
muscle).
CLINICAL FEATURES
11.
Cold ,clammy skin.
Threadyperipheral pulses .
Distended neck vein.
Tachypnea, with respiratory crackles.
cyanosis.
sweating, cold hand and feet
.
The goal ofmedical management in cardiogenic shock
are.
1. To limit further myocardial damage and preserve the
healthy myocardium. ( To improve blood flow to
myocardium)
2. To improve the cardiac function by increasing cardiac
contractility, decreasing ventricular after load or both.
In general this goals are achieved by increasing oxygen
supply to the heart muscle while reducing oxygen
demands.
GOAL
16.
First line treatmentof cardiogenic shock involves
the following actions.
1. Supplying supplemental oxygen
2. Controlling chest pain
3. Providing selected fluid support
4. Administrating vasoactive medications
First-line treatment
17.
Oxygen is administratedat a rate 2 to 6
L/Min to achieve oxygen saturation above
90 %.
Monitoring of ABG Value and pulse
oximetry help
to determine if patient require more
oxygen therapy.
Pain Control
Morphine sulphate ( IV)
Oxygen therapy
Percutaneous coronary intervention
CoronaryArtery bypass graft
Intra – aortic Balloon Pump ( IABP)
Transvenous pacing
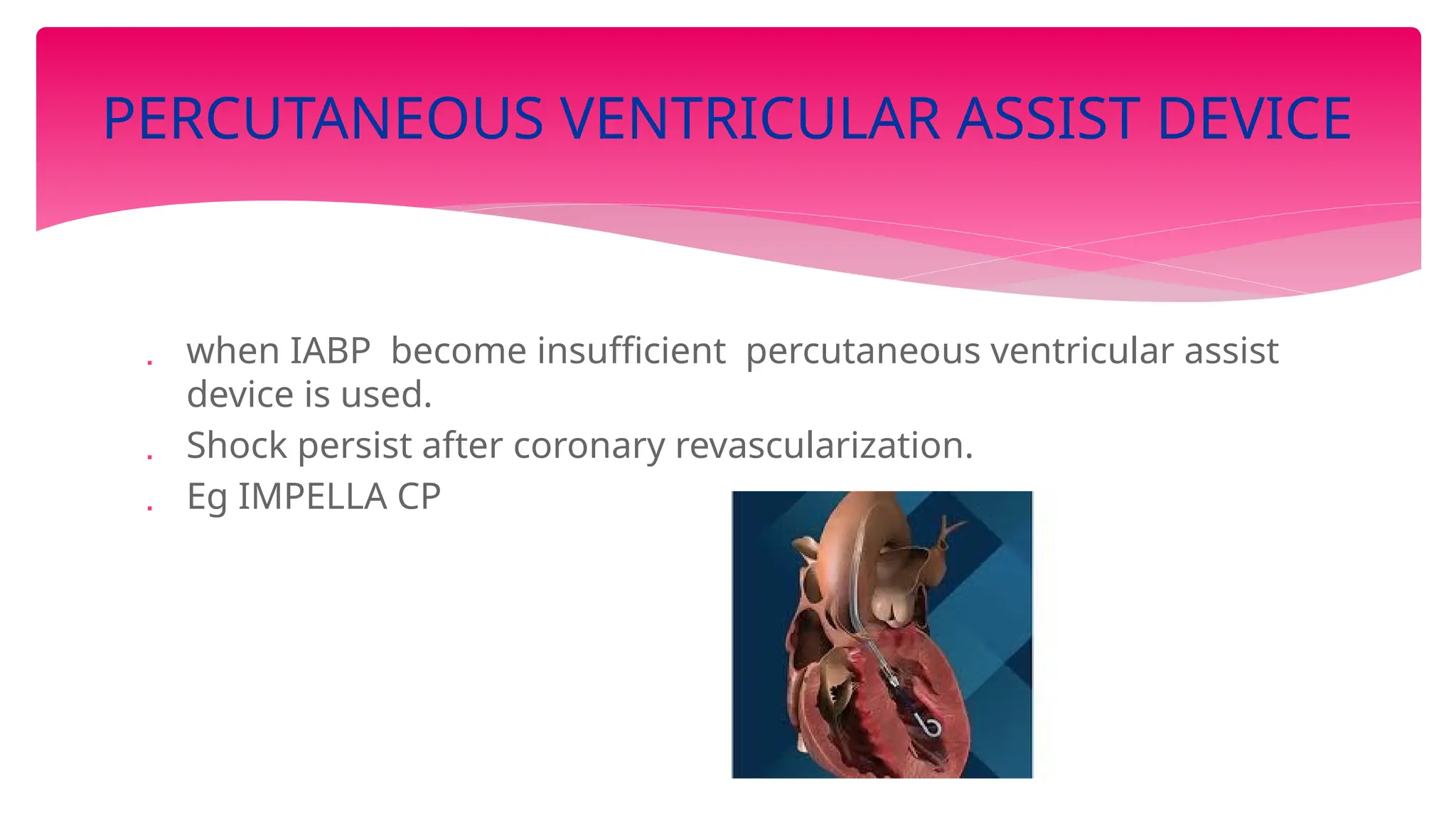
Percutaneous Ventricular Assist Device.
Extracorporeal Membrane oxygenation
Short or Long Term Left ventricular
assist Device
PROCEDURES
22.
PCI isrecommended for Patient with acute MI
followed by cardiogenic shock.
Percutaneous coronary intervention is performed
by inserting a catheter through the skin in the
groin or arm into an artery.
At the leading tip of this catheter, several different
devices such as a balloon,Stent or cutting device
(artherectomy device) can be deployed.
The catheter and its devices are threaded
through the inside of the artery back into an area
of coronary artery narrowing or blockage.
PERCUTANEOUS CORONARY INTERVENTION
( PCI)
23.
IABP Isa device used for mechanical circulatory
assistance in case of LV dysfunction on the
principle of counter pulsation
1. The goals of IABP include the following..
2. Increased SV
3. Improved coronary artery perfusion Decreased
preload
4. Decreased cardiac work load
INTRAAROTIC BALLON PUMP
24.
IABP Consistof intra aortic balloon about 1o
inches long placed over the distal end of
catheter.
Catheter is inserted surgically or percutaneously
over femoral artery.
When it reaches in aorta ,tip of balloon is
positioned just below the tip of the origin of left
subclavian artery.
PROCEDURE
25.
Pump consolemonitor the patient’s heartbeat
R Wave in the ECG trigger pumps inflating mechanism
As balloon inflates it displaces the blood, increase aortic
pressure, which increase coronary blood flow.
During left ventricular ejection balloon deflates, thus reducing
aortic pressure, help in ejection of blood from left ventricle,
reducing workload of left ventricle.
.
coronary arterybypass graft (CABG) surgeries are
among the most commonly performed major
operations.
CABG surgery is advised for selected groups of
patients with significant narrowing and
blockages of the heart arteries (coronary artery
disease , cardiogenic shock).
CABG surgery creates new routes around
narrowed and blocked arteries, allowing
sufficient blood flow to deliver oxygen and
nutrients to the heart muscle.(saphenous vein,
mammary or radial artery)
CORONARY ARTERY BYPASS GRAFT
31.
Provides hemodynamicsupport
and oxygenation if Heart / lung
function is compromised.
EXTRACORPOREAL MEMBRANE
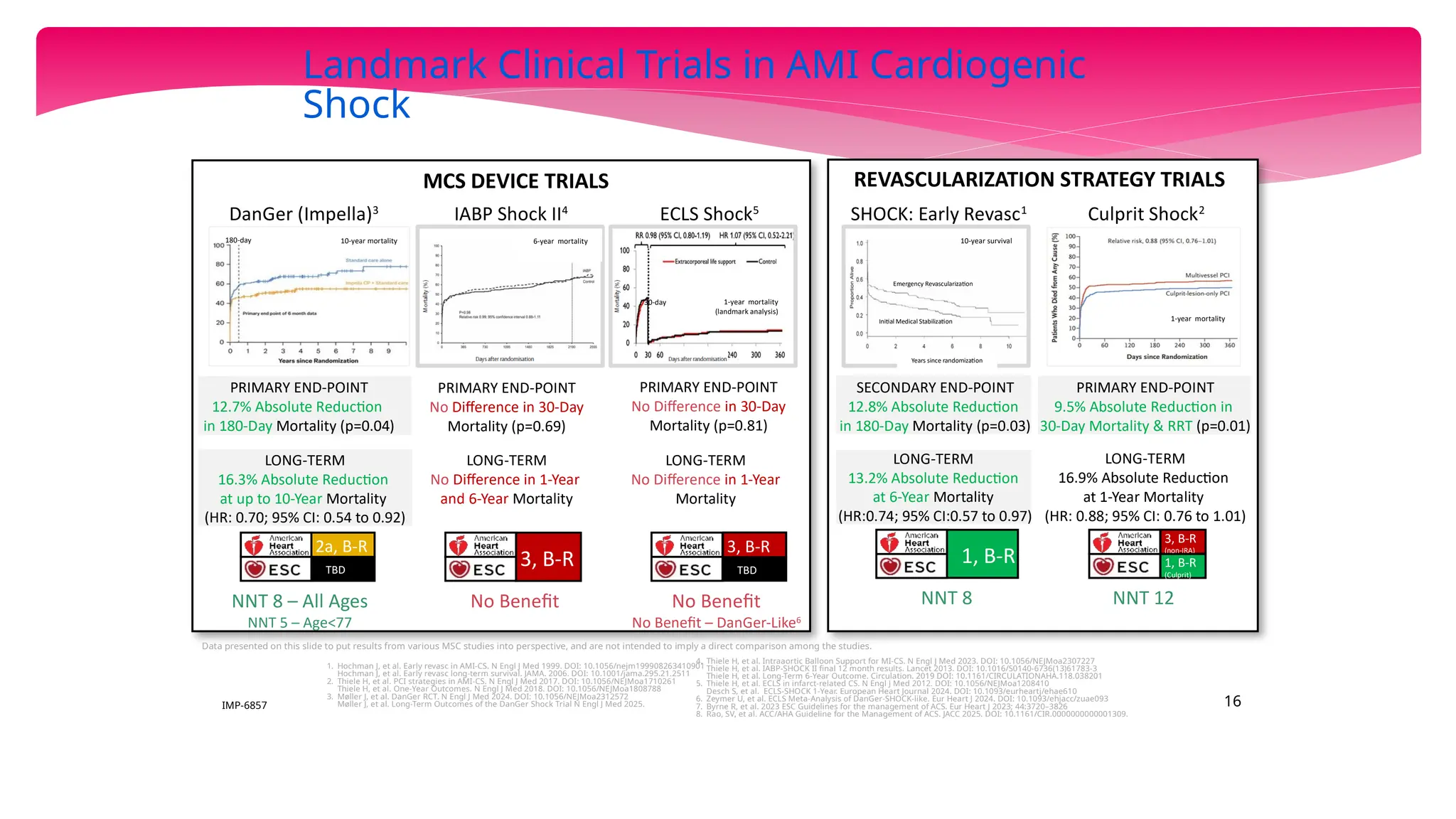
SHOCK: Early Revasc1
LandmarkClinical Trials in AMI Cardiogenic
Shock
REVASCULARIZATION STRATEGY TRIALS
MCS DEVICE TRIALS
PRIMARY END-POINT
12.7% Absolute Reduction
in 180-Day Mortality (p=0.04)
DanGer (Impella)3
PRIMARY END-POINT
No Difference in 30-Day
Mortality (p=0.81)
IABP Shock II4
Culprit Shock2
PRIMARY END-POINT
No Difference in 30-Day
Mortality (p=0.69)
PRIMARY END-POINT
9.5% Absolute Reduction in
30-Day Mortality & RRT (p=0.01)
LONG-TERM
16.9% Absolute Reduction
at 1-Year Mortality
(HR: 0.88; 95% CI: 0.76 to 1.01)
SECONDARY END-POINT
12.8% Absolute Reduction
in 180-Day Mortality (p=0.03)
LONG-TERM
13.2% Absolute Reduction
at 6-Year Mortality
(HR:0.74; 95% CI:0.57 to 0.97)
1. Hochman J, et al. Early revasc in AMI-CS. N Engl J Med 1999. DOI: 10.1056/nejm199908263410901
Hochman J, et al. Early revasc long-term survival. JAMA. 2006. DOI: 10.1001/jama.295.21.2511
2. Thiele H, et al. PCI strategies in AMI-CS. N Engl J Med 2017. DOI: 10.1056/NEJMoa1710261
Thiele H, et al. One-Year Outcomes. N Engl J Med 2018. DOI: 10.1056/NEJMoa1808788
3. Møller J, et al. DanGer RCT. N Engl J Med 2024. DOI: 10.1056/NEJMoa2312572
Møller J, et al. Long-Term Outcomes of the DanGer Shock Trial N Engl J Med 2025.
4. Thiele H, et al. Intraaortic Balloon Support for MI-CS. N Engl J Med 2023. DOI: 10.1056/NEJMoa2307227
Thiele H, et al. IABP-SHOCK II final 12 month results. Lancet 2013. DOI: 10.1016/S0140-6736(13)61783-3
Thiele H, et al. Long-Term 6-Year Outcome. Circulation. 2019 DOI: 10.1161/CIRCULATIONAHA.118.038201
5. Thiele H, et al. ECLS in infarct-related CS. N Engl J Med 2012. DOI: 10.1056/NEJMoa1208410
Desch S, et al. ECLS-SHOCK 1-Year. European Heart Journal 2024. DOI: 10.1093/eurheartj/ehae610
6. Zeymer U, et al. ECLS Meta-Analysis of DanGer-SHOCK-like. Eur Heart J 2024. DOI: 10.1093/ehjacc/zuae093
7. Byrne R, et al. 2023 ESC Guidelines for the management of ACS. Eur Heart J 2023; 44:3720–3826
8. Rao, SV, et al. ACC/AHA Guideline for the Management of ACS. JACC 2025. DOI: 10.1161/CIR.0000000000001309.
1, B-R
3, B-R
NNT 12
NNT 8
NNT 8 – All Ages
NNT 5 – Age<77
Data presented on this slide to put results from various MSC studies into perspective, and are not intended to imply a direct comparison among the studies.
LONG-TERM
No Difference in 1-Year
and 6-Year Mortality
EXTENDED END-POINT
No Difference in 180-Day
Mortality (p=0.91)
TBD
2a, B-R
No Benefit No Benefit
No Benefit – DanGer-Like6
3, B-R
(non-IRA)
1, B-R
(Culprit)
TBD
3, B-R
180-day 10-year mortality
LONG-TERM
16.3% Absolute Reduction
at up to 10-Year Mortality
(HR: 0.70; 95% CI: 0.54 to 0.92)
6-year mortality
ECLS Shock5
1-year mortality
(landmark analysis)
30-day
LONG-TERM
No Difference in 1-Year
Mortality
Years since randomization
Emergency Revascularization
Initial Medical Stabilization
10-year survival
1-year mortality
16
IMP-6857
34.
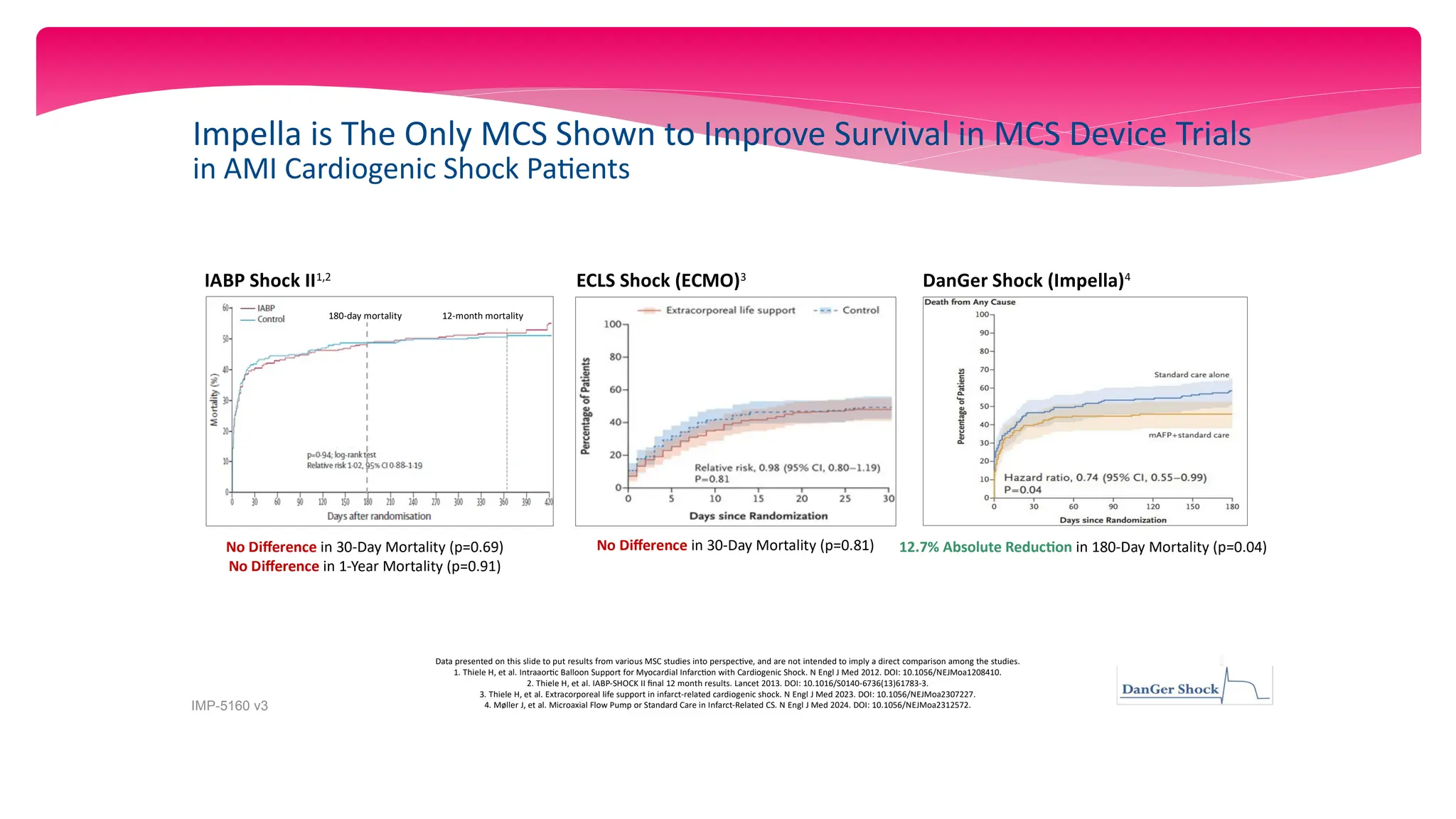
Impella is TheOnly MCS Shown to Improve Survival in MCS Device Trials
in AMI Cardiogenic Shock Patients
12.7% Absolute Reduction in 180-Day Mortality (p=0.04)
DanGer Shock (Impella)4
No Difference in 30-Day Mortality (p=0.81)
ECLS Shock (ECMO)3
IABP Shock II1,2
No Difference in 30-Day Mortality (p=0.69)
No Difference in 1-Year Mortality (p=0.91)
Data presented on this slide to put results from various MSC studies into perspective, and are not intended to imply a direct comparison among the studies.
1. Thiele H, et al. Intraaortic Balloon Support for Myocardial Infarction with Cardiogenic Shock. N Engl J Med 2012. DOI: 10.1056/NEJMoa1208410.
2. Thiele H, et al. IABP-SHOCK II final 12 month results. Lancet 2013. DOI: 10.1016/S0140-6736(13)61783-3.
3. Thiele H, et al. Extracorporeal life support in infarct-related cardiogenic shock. N Engl J Med 2023. DOI: 10.1056/NEJMoa2307227.
4. Møller J, et al. Microaxial Flow Pump or Standard Care in Infarct-Related CS. N Engl J Med 2024. DOI: 10.1056/NEJMoa2312572.
IMP-5160 v3
12-month mortality
180-day mortality
35.
Heart Recovery
IMP-6064 v3
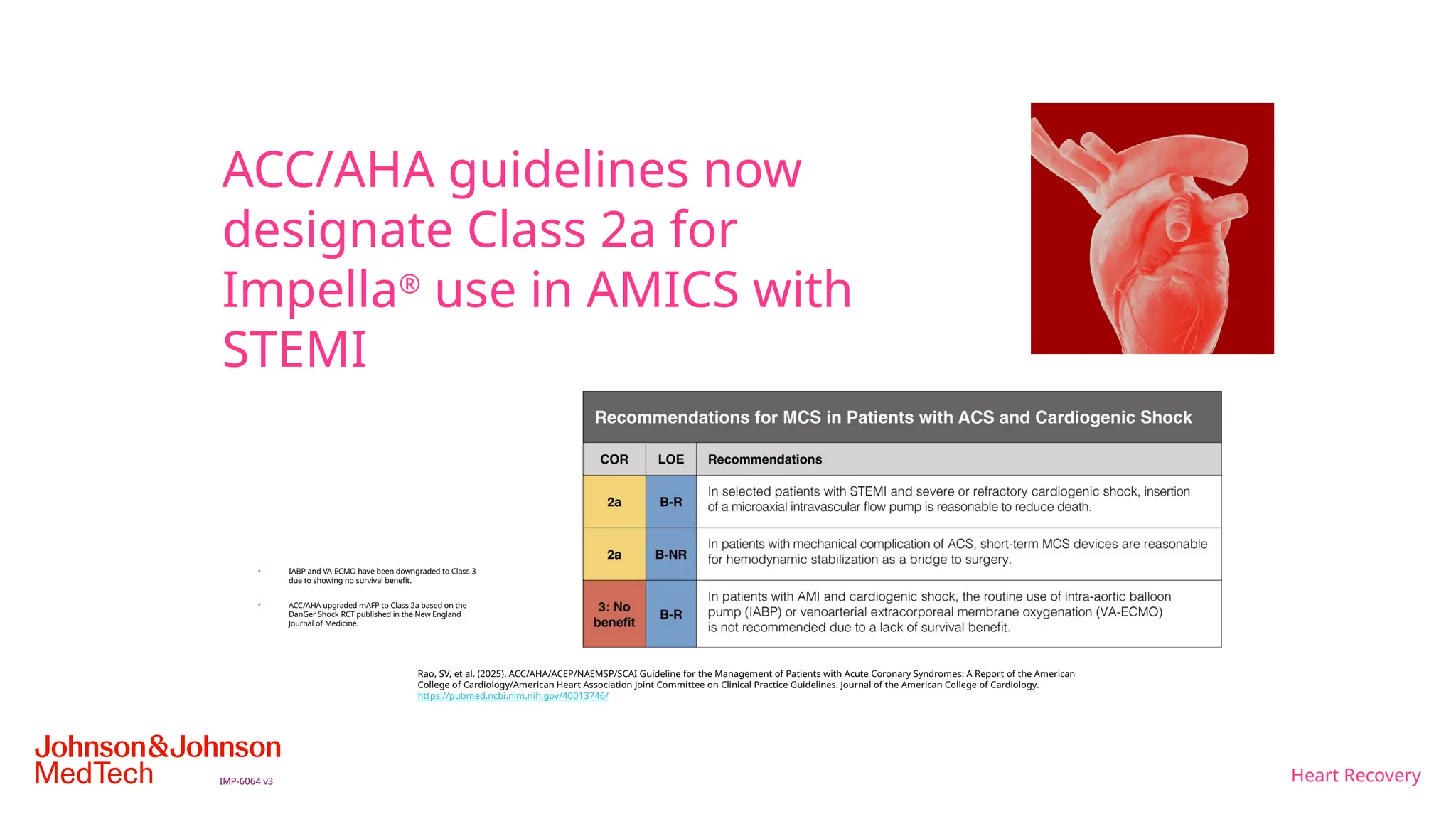
ACC/AHAguidelines now
designate Class 2a for
Impella®
use in AMICS with
STEMI
• IABP and VA-ECMO have been downgraded to Class 3
due to showing no survival benefit.
• ACC/AHA upgraded mAFP to Class 2a based on the
DanGer Shock RCT published in the New England
Journal of Medicine.
Rao, SV, et al. (2025). ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients with Acute Coronary Syndromes: A Report of the American
College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Journal of the American College of Cardiology.
https://pubmed.ncbi.nlm.nih.gov/40013746/
NURSING ASSESSMENT.
Administersafe and accurate IV fluids and medications.
Documents and records medications and treatment that
are administered as well as the patient response to
treatment.
Patients receiving thrombolytic therapy must be
monitored for bleeding. Arterial and venous puncture
sites must be observed for bleeding, and pressure must
be applied at the sites if bleeding occurs.
.
Nursing management
38.
Neurologic assessment isessential after the
administration of thrombolytic therapy to assess for the
potential complications of cerebral haemorrhage
associated with the therapy.
Urine output ,BUN ,creatinine levels should be
monitored.
Maintain mechanical assistive devices function Prevent
complications associated with cardiogenic shock.
Enhancing safety and comfort.
.
39.
Decreased cardiacoutput related to impaired
contractility due to extensive heart muscle damage.
GOAL
Improving cardiac output
INTERENTION
Establish continuous ECG monitoring
Hemodynamic monitoring
Closely monitor adverse response to drug therapy
Monitor BP with intra-arterial line continuously.
Measure and record intake and urine out put
NURSING DIAGNOSIS
40.
GOAL :Improvingoxygenation
INTERVENTION
1. Monitor rate and rhythm of respiratory every hour. *
Auscultation lung fields for abnormal sounds * ABG evaluation *
2. Administer oxygen * Invasive oxygen therapies (ET & MV)
Impaired gas exchange related to pulmonary
congestion due to elevated left ventricular pressure
41.
GOAL :Maintaining adequate Tissue perfusion
INTERVENTION
Perform neurologic assessment every hour using with “Glasgow
coma scale” ( GCS)
Report changes immediately
Obtain BUN & creatinine blood levels & monitor output to
evaluate renal function.
Ineffective tissue perfusion ( renal,
cerebral, cardiopulmonary GI and
peripheral) related to decreased blood
flow
42.
Goal : ToRelive anxiety
Assess the anxiety level
Provide adequate information regarding
physical condition
Encourage to ask questions
Provide diverational therapy
Anxiety related to intensive care environment and invasive procedures.
Summary & Takeaways
Shock classification dictates treatment mismanagement can
worsen outcomes.
Cardiogenic shock demands rapid intervention and
continuous monitoring.
Combination of vasopressors, inotropes, and devices tailored
to each patient.
Emerging drugs and MCS support devices hold promise for
refractory cases.
45.
Cardiogenic shock isa treatable illness with a
reasonable chance for full recovery. The
Cardiogenic shock literature has traditionally
focused on the very high mortality associated
with this diagnosis. It is important to
recognize that although patients with
Cardiogenic shock are at very high risk for
early death, great potential exists for salvage.
CONCLUSION
46.
Chintamani, Lewis, Textbook of Medical
surgical Nursing, Elsevier Publication 13 th
edition. volume 1. 2011.pg no 1723-1725.
Black.M.Joyce.Text book of Medical SurgIcal
N.Elsevier Publication.8 th edition .PG . No 2134
3136.
Griffin .P.Brain, Manaul of Cardiovascular
Medicine. Lippincott punbllication.4 th edition.
volume 1. pg no 77 to 80.
BIBILIOGRAPHY