Importance of Lipidsand Lipoproteins
Physiologic:
• Cholesterol & phospholipids are vital structural components of cellular membranes.
• Cholesterol is the precursor of steroid hormones and bile acids
• Triglyceride is an important storage and transport form of energy
• Absorption of dietary lipid is essential for the absorption of fat-soluble vitamins
3.
Importance of Lipidsand Lipoproteins
Pathologic
• Hypercholesterolaemia (and to a lesser extent hypertriglyceridaemia) is associated
with an increased risk of developing atherosclerosis.
• Hypertriglyceridaemia predisposes patients to pancreatitis
• Rare inherited defects of lipid metabolism occur, causing significant morbidity and
mortality.
4.
The Major Lipidsin Plasma
Sterol lipids (22%)
- Cholesterol and Cholesterol Ester
• can be synthesized de novo from acetyl Co-A in the liver.
• The rate-limiting step is catalysed by HMG-CoA reductase .
• Also derived from ‘animals’ in diet. Cf Plants Sterols
Glycerol Lipids (14%)
- Triglycerides
• Endogenous source - liver which utilises fatty acids
• Exogenous source derived from dietary fatty acids
5.
The Major Lipidsin Plasma
Sphingolipids (35%)
Sphingomyelin
Glycerolphospholipids (29%)
Phosphatidylcholine, Phosphatidylethanolamine
Fatty Acyls (<1%)
Fatty Acids
All of these lipids can be measured in plasma…depending on the clinical
indication
6.
Lipid Transport inthe Plasma
Lipids are relatively insoluble in water
They are transported in the aqueous environment of the plasma as lipoproteins.
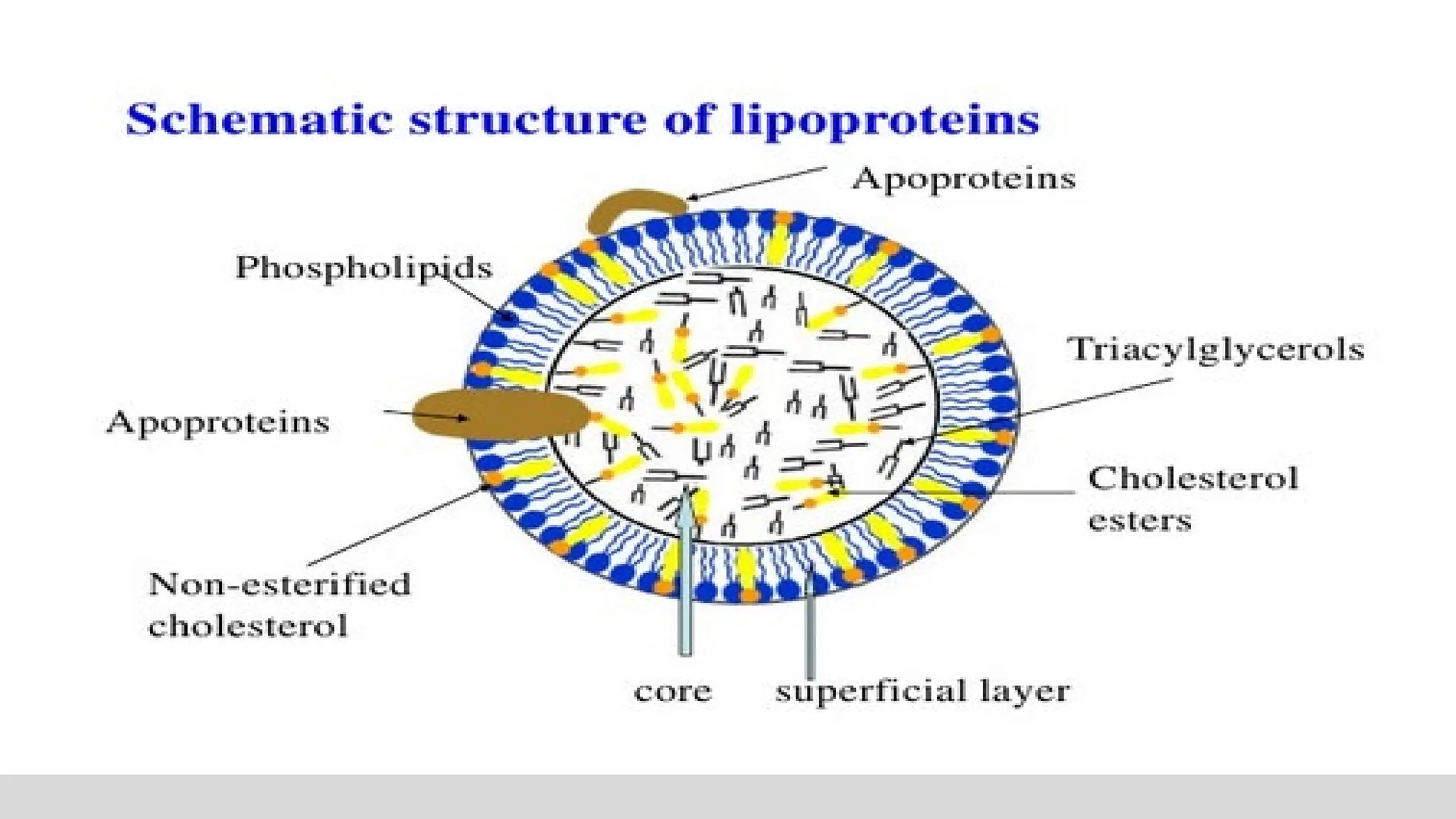
Lipoproteins
Macromolecular complexes that are soluble in plasma and contain an internal core of
lipids. They consists of esterified and unesterified cholesterol, triglycerides,
phospholipids and apolipoproteins.
Apolipoprotein
The protein constituent of lipoproteins. Apolipoproteins play a role in assembly and
secretion of lipoproteins, provide structural integrity, activate or inhibit enzymes and act
as ligands for specific receptors, mitigating uptake of particles or lipid components.
8.
Lipoprotein Metabolic Pathways
•Exogenous cholesterol transport for delivery of dietary lipids to the tissues
• Permits efficient transport of dietary lipids…energy to the tissues without going thro
the liver.
• Endogenous cholesterol transport for delivery of hepatic lipids to the tissues
• Permits the delivery of cholesterol to the tissues….more efficient for tissues to
receive cholesterol than to make cholesterol
• Reverse cholesterol transport
• Cholesterol in peripheral cells is transported from the plasma membranes of
peripheral cells to the liver and intestine
9.
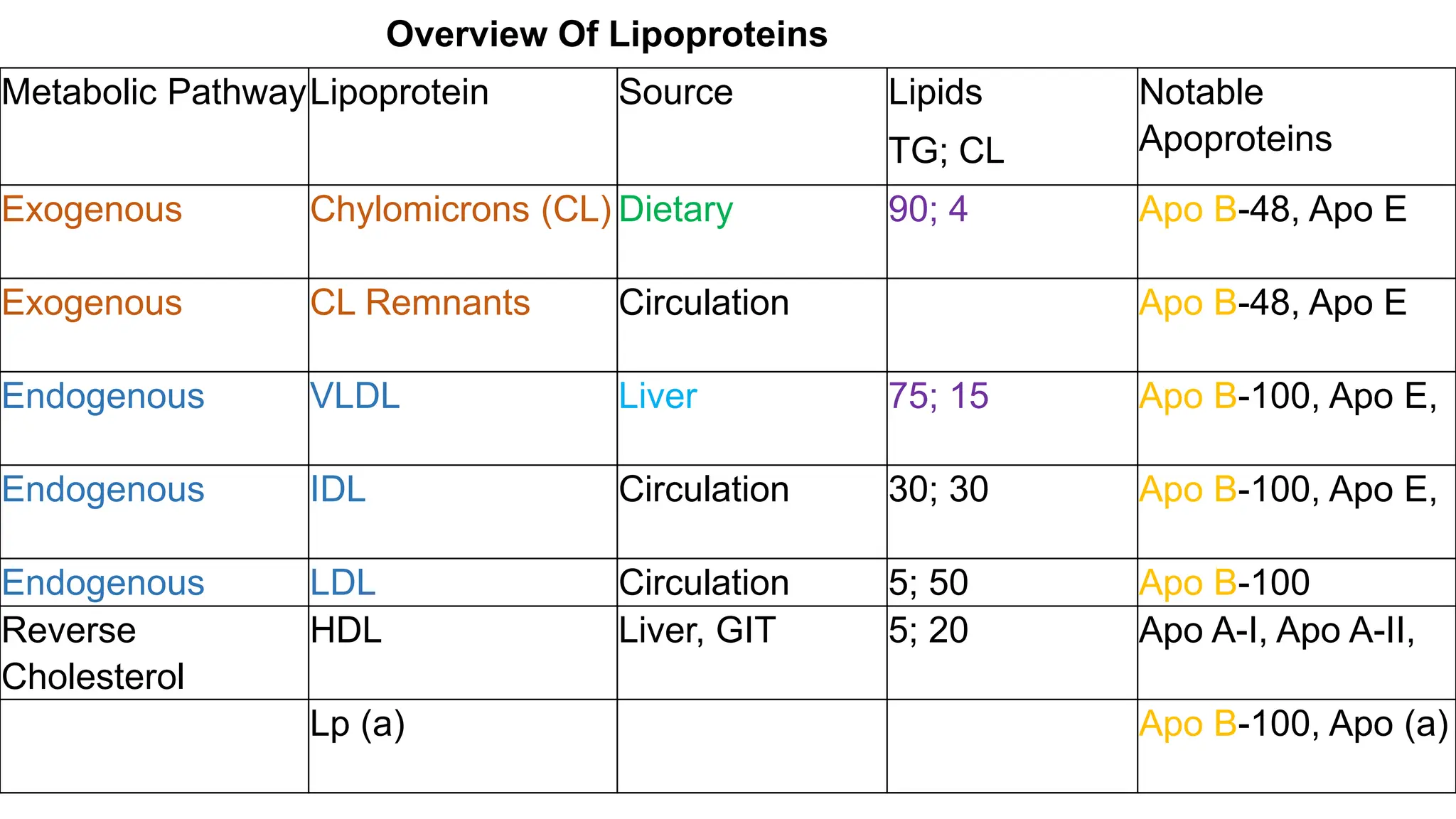
Metabolic PathwayLipoprotein SourceLipids
TG; CL
Notable
Apoproteins
Exogenous Chylomicrons (CL) Dietary 90; 4 Apo B-48, Apo E
Exogenous CL Remnants Circulation Apo B-48, Apo E
Endogenous VLDL Liver 75; 15 Apo B-100, Apo E,
Endogenous IDL Circulation 30; 30 Apo B-100, Apo E,
Endogenous LDL Circulation 5; 50 Apo B-100
Reverse
Cholesterol
HDL Liver, GIT 5; 20 Apo A-I, Apo A-II,
Lp (a) Apo B-100, Apo (a)
Overview Of Lipoproteins
10.
Atherosclerotic Cardiovascular Disease
Atherosclerosisrefers to the underlying disorder involving the intima of medium size and
large arteries, which leads to the accumulation of lipid, mainly cholesterol and
cholesterol laden macrophages (foam cells), and the development of a raised fibrous
lesion.
Atherosclerosis of the
• coronary arteries auses myocardial infarction & angina pectoris
• arteries supplying the central nervous system provokes strokes and TIA
• peripheral circulation causes intermittent claudication and gangrene
• splanchnic circulation can cause mesenteric ischemia.
• Kidneys can cause renal artery stenosis
11.
Lipids and AtheroscleroticCardiovascular Disease
• Retention of apoB-containing lipoproteins in the subendothelial space is an initial step
• Modification (oxidation, glycation), of retained lipoproteins drives activation of
endothelial cells.
• Activated cells increase expression of monocyte interaction/adhesion molecules &
chemoattractants with attachment/transmigration of monocytes into the intimal space.
• Monocytes differentiate into macrophages and express receptors that mediate the
internalization of VLDL, APOE remnants, and modified LDL to become foam cells.
• In addition, inflammatory signaling pathways are activated in macrophage foam cells
leading to more cell recruitment and LDL modification.
12.
Atherogenic and Anti-AtherogenicLipoproteins
Atherogenic lipoproteins – lipoproteins which increase the risk of the development of
atherosclerosis
- ApoB containing – VLDL, IDL, LDL, Lipoprotein (a)
Anti-atherogenic lipoproteins - lipoproteins which decrease the risk of the development
of atherosclerosis
- HDL
13.
Assessment for riskof ASCVD
Lipid Profile
Standard panel
• Total Cholesterol – all the cholesterol in all the lipoproteins in plasma
• Triglycerides – all the triglycerides in all the lipoproteins in plasma
• HDL-cholesterol – the cholesterol in high density lipoprotein in plasma
surrogate of HDL
• LDL- cholesterol – the cholesterol in low density lipoprotein in plasma
surrogate of LDL
14.
Assessment for disordersof Lipid Metabolism
LDL-cholesterol
• Primary cause of atherosclerosis
• Used to define statin benefit group
• Used to define treatment targets
• Unlike the other parameters, it is not easily and accurately measured directly
• Usually determined by calculation from the concentration of TC, HDL-C and TG
determined from fasting samples
• Friedewald formula
• Martins-Hopkins Equation
• Sampson NIH equation
15.
Assessment for disordersof Lipid Metabolism
Friedewald Formula
• LDL-C = TC – (TG/5 + HDL-C) [mg/dL]
• Requirements
• Triglyceride to Cholesterol ratio in Very Low Density Lipoprotein (VLDL) is relatively
constant in normal subjects and nearly all patients with dyslipidemia at about 5:1
• When chylomicrons are not detectable in the blood, most of the triglyceride in
plasma is from VLDL (Fasting – 12 hours)
• Not accurate when TG is greater than 400mg/dL
• Not reliable when LDL-C is less than 70mg/dL
16.
Assessment for disordersof Lipid Metabolism
• Extended Martins-Hopkins Equation
• Sampson NIH equation
• Applicable up to TG < 800mg/dL
• Calculation requires Apps or online calculators
• There are other equations…
17.
Assessment for disordersof Lipid Metabolism
Non-high-density Lipoprotein Cholesterol (Non-HDL-C)
• represents the cholesterol contained in all lipoproteins except HDL-C and it can be
calculated from the standard lipid panel by subtracting HDL-C from total cholesterol.
• It represents the cholesterol content present in all atherogenic lipoproteins and serves
as a better surrogate for the overall atherogenic burden than LDL-C alone, making it a
useful marker in the assessment of CVD risk.
• May also be used as a target of therapy
18.
Assessment for disordersof Lipid Metabolism
Plasma Apolipoprotein B
• present on atherogenic lipoproteins and serves as a macromolecular scaffold to
provide structural integrity. I
• t also serves as a ligand for the LDL receptor, which facilitates its clearance from the
plasma.
• There are two major isoforms of apoB: apoB48, found on intestinally derived
lipoproteins (chylomicrons and their remnants) and apoB100, found on hepatically
derived lipoproteins – very LDL, intermediate-density lipoprotein, LDL and lipoprotein
(a) (Lp[a]).
.
19.
Assessment for disordersof Lipid Metabolism
Plasma Apolipoprotein B
• Each of these atherogenic particles harbours single copy of apoB.
• Thus, apoB represents a better proxy of total atherogenic lipoprotein particle
concentration
• Target of therapy and risk assessment
.
20.
Assessment for disordersof Lipid Metabolism
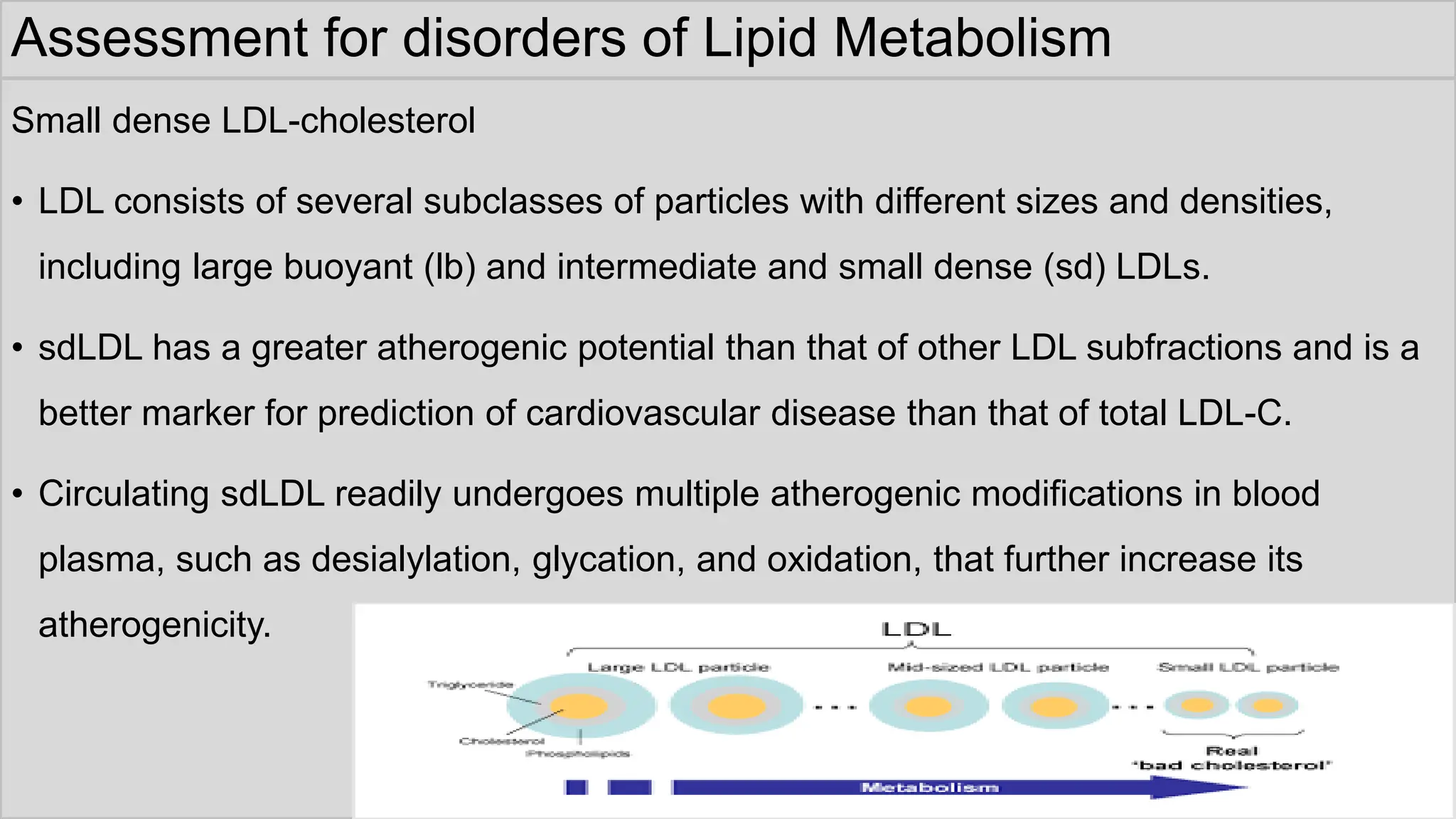
Small dense LDL-cholesterol
• LDL consists of several subclasses of particles with different sizes and densities,
including large buoyant (lb) and intermediate and small dense (sd) LDLs.
• sdLDL has a greater atherogenic potential than that of other LDL subfractions and is a
better marker for prediction of cardiovascular disease than that of total LDL-C.
• Circulating sdLDL readily undergoes multiple atherogenic modifications in blood
plasma, such as desialylation, glycation, and oxidation, that further increase its
atherogenicity.
21.
Assessment for disordersof Lipid Metabolism
Low-density Lipoprotein Particle Number
• LDL particle (LDL-P) number represents an alternative to LDL-C as a marker of CVD
risk.
• LDL-P represents the concentration in nanomoles of LDL particles per litre of plasma
volume, LDL-C represents the cholesterol mass in milligrams found in LDL particles in
a decilitre of plasma.
.
22.
Assessment for disordersof Lipid Metabolism
Lipoprotein(a)
• Lp(a) consists of a molecule of apolipoprotein(a) – apo(a) – a non- functional mimic of
plasminogen, covalently bound to apoB on an LDL-like particle.
• Significant heterogeneity between apo(a) isoforms confers heterogeneity in Lp(a)
particles.
• Plasma concentration of Lp(a) is >90% genetically determined in an autosomal co-
dominant fashion, with adult levels achieved by about 5 years of age.
• Lp(a) levels remain stable throughout life regardless of lifestyle.
23.
Lipids and AtheroscleroticCardiovascular Disease
• Lifestyle Risk Factors
• Obesity (BMI ≥30 Kg/M2)
• Physical Inactivity
• Atherogenic Diet
• Emerging Risk Factors
• Lipoprotein (A)
• Prothrombotic Factors
• Proinflammatory Factors
• Impaired Fasting Glucose
• Subclinical Atherosclerosis
• High LDL Cholesterol
• Low HDL Cholesterol
• <40 mg/dL
• Cigarette Smoking
• Hypertension
• BP ≥140/90 mmHg or On AntiHTsive
• Diabetes Mellitus
• Family History Of Premature CHD
• Age
• Men ≥45yrs; Women ≥55yrs
• Stage 3 or 4 chronic kidney disease
Apart from disorders of cholesterol, other risk factors exist for the development of ASCVD
24.
Lipids and AtheroscleroticCardiovascular Disease
• At the very heart of primary prevention is the identification of individuals at-risk of
atherosclerotic cardiovascular disease
• This requires a consideration of all risk factors…NOT JUST plasma lipids.
• CVD risk prediction equations allow for the combination of all the major risk factors
1) Report a single numerical risk estimate for the individual – 10 year risk
2) Next step is to categorise risk level
• Numerical estimate and risk categorization varies with the equation used
25.
CVD risk predictionequations
• CVD risk equations (requires an APP or online calculator)
• Predicting Risk of cardiovascular disease EVENTs (PREVENT)
• Estimates the 10- and 30-year risk of heart attack and stroke for people aged 30 years and older
• Pooled Cohort Equations
• Estimate the 10-year primary risk of ASCVD among patients without pre-existing cardiovascular
disease who are between 40 and 79 years of age.
• Framingham Risk Score for Hard Coronary Heart Disease
• for use in non-diabetic patients age 30-79 years with no prior history of coronary heart disease or
intermittent claudication
• Systematic Coronary Risk Evaluation 2 (SCORE2)
• Predicts 10-year CVD risk in patients without prior CVD or diabetes
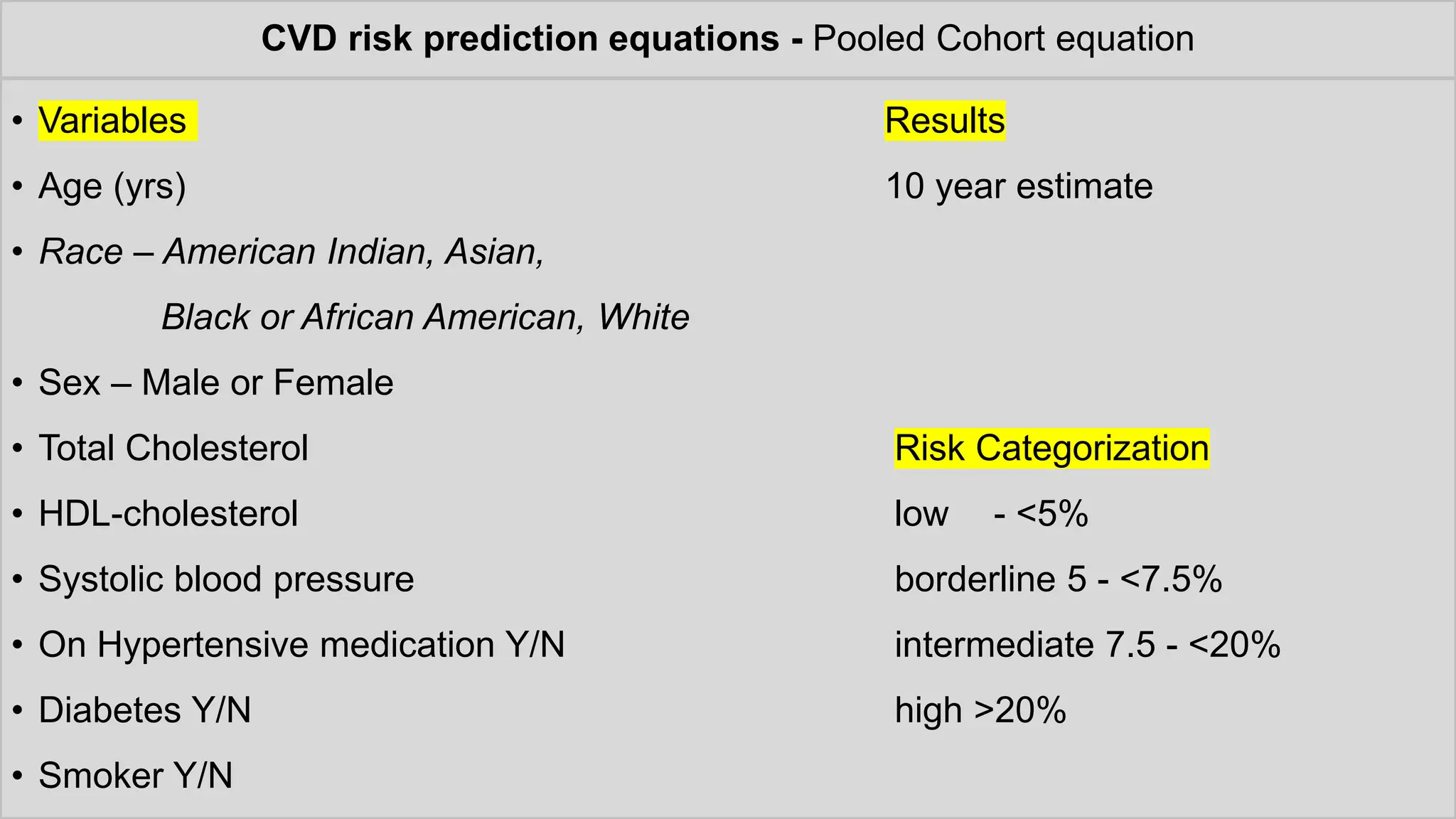
CVD risk predictionequations - Pooled Cohort equation
• Variables Results
• Age (yrs) 10 year estimate
• Race – American Indian, Asian,
Black or African American, White
• Sex – Male or Female
• Total Cholesterol Risk Categorization
• HDL-cholesterol low - <5%
• Systolic blood pressure borderline 5 - <7.5%
• On Hypertensive medication Y/N intermediate 7.5 - <20%
• Diabetes Y/N high >20%
• Smoker Y/N
29.
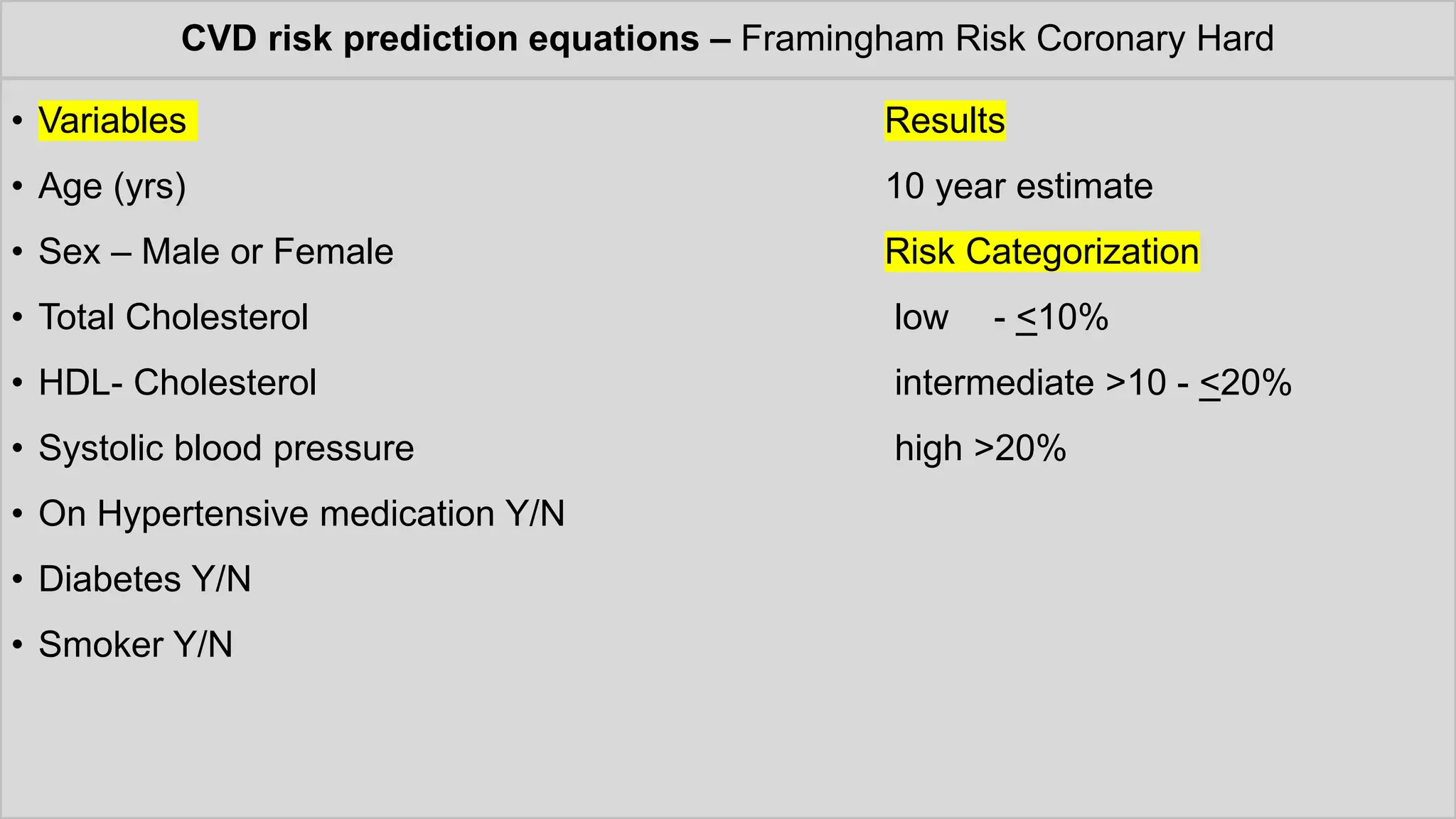
CVD risk predictionequations – Framingham Risk Coronary Hard
• Variables Results
• Age (yrs) 10 year estimate
• Sex – Male or Female Risk Categorization
• Total Cholesterol low - <10%
• HDL- Cholesterol intermediate >10 - <20%
• Systolic blood pressure high >20%
• On Hypertensive medication Y/N
• Diabetes Y/N
• Smoker Y/N
30.
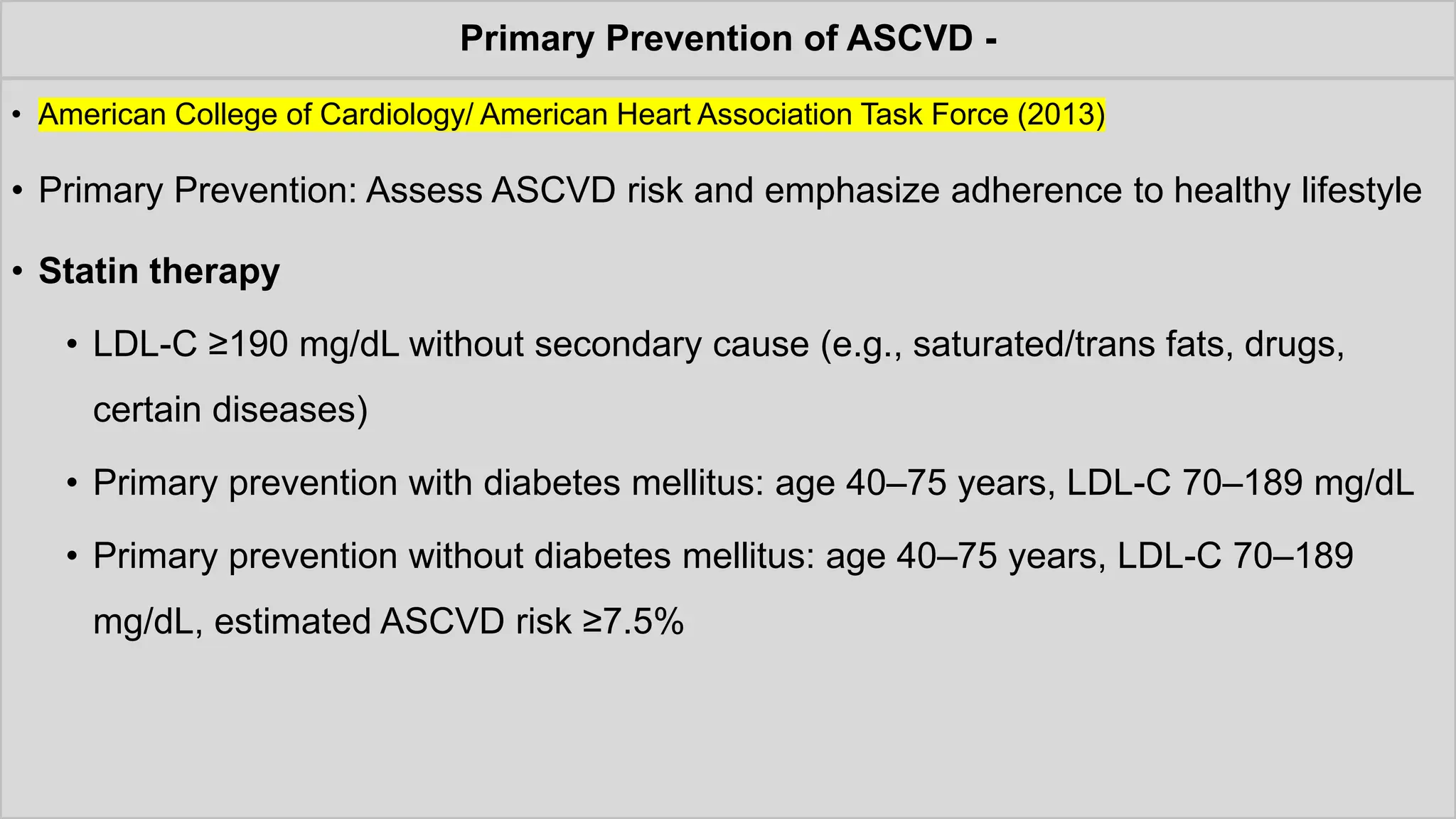
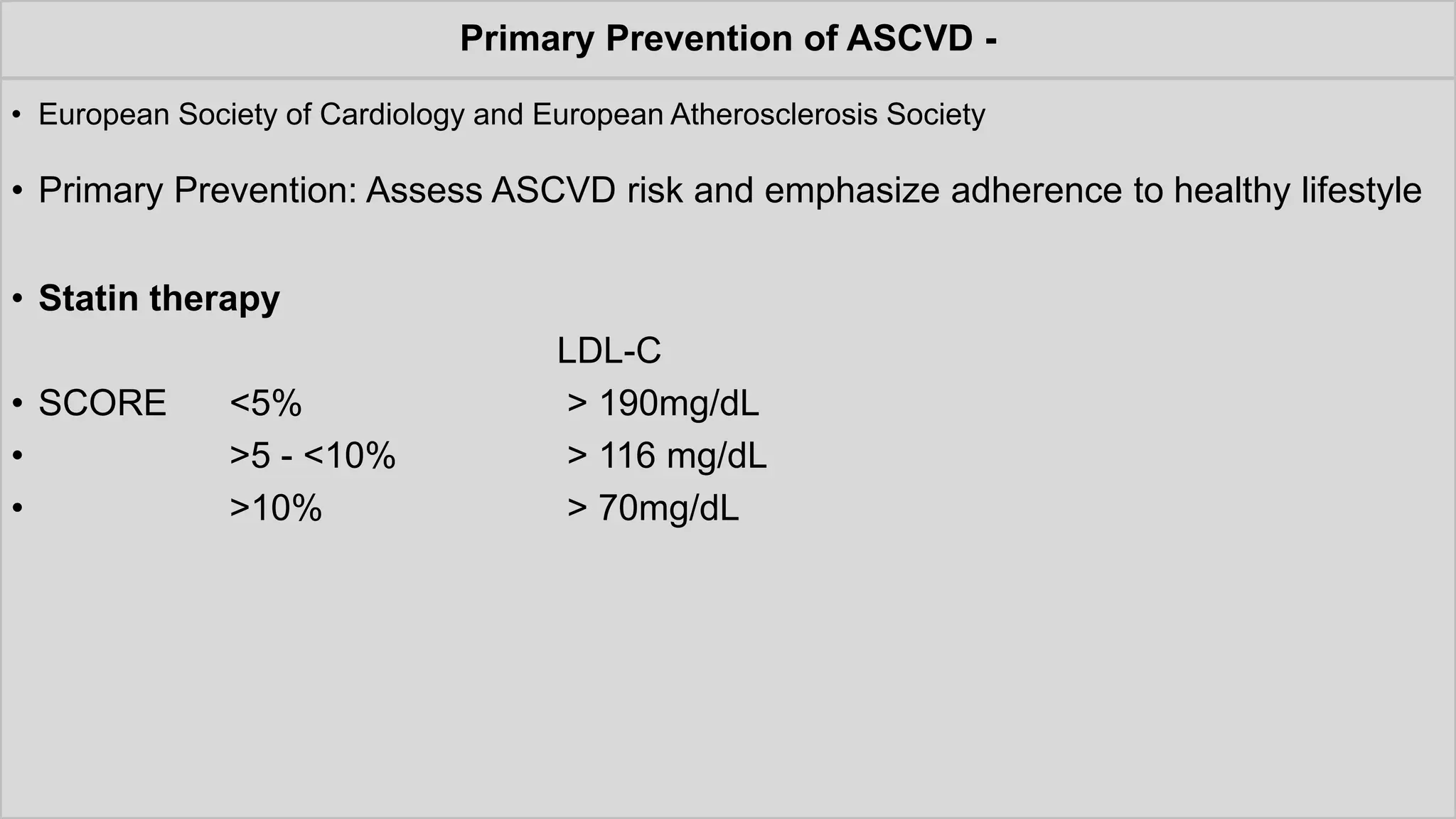
Primary Prevention ofASCVD -
• American College of Cardiology/ American Heart Association Task Force (2013)
• Primary Prevention: Assess ASCVD risk and emphasize adherence to healthy lifestyle
• Statin therapy
• LDL-C ≥190 mg/dL without secondary cause (e.g., saturated/trans fats, drugs,
certain diseases)
• Primary prevention with diabetes mellitus: age 40–75 years, LDL-C 70–189 mg/dL
• Primary prevention without diabetes mellitus: age 40–75 years, LDL-C 70–189
mg/dL, estimated ASCVD risk ≥7.5%
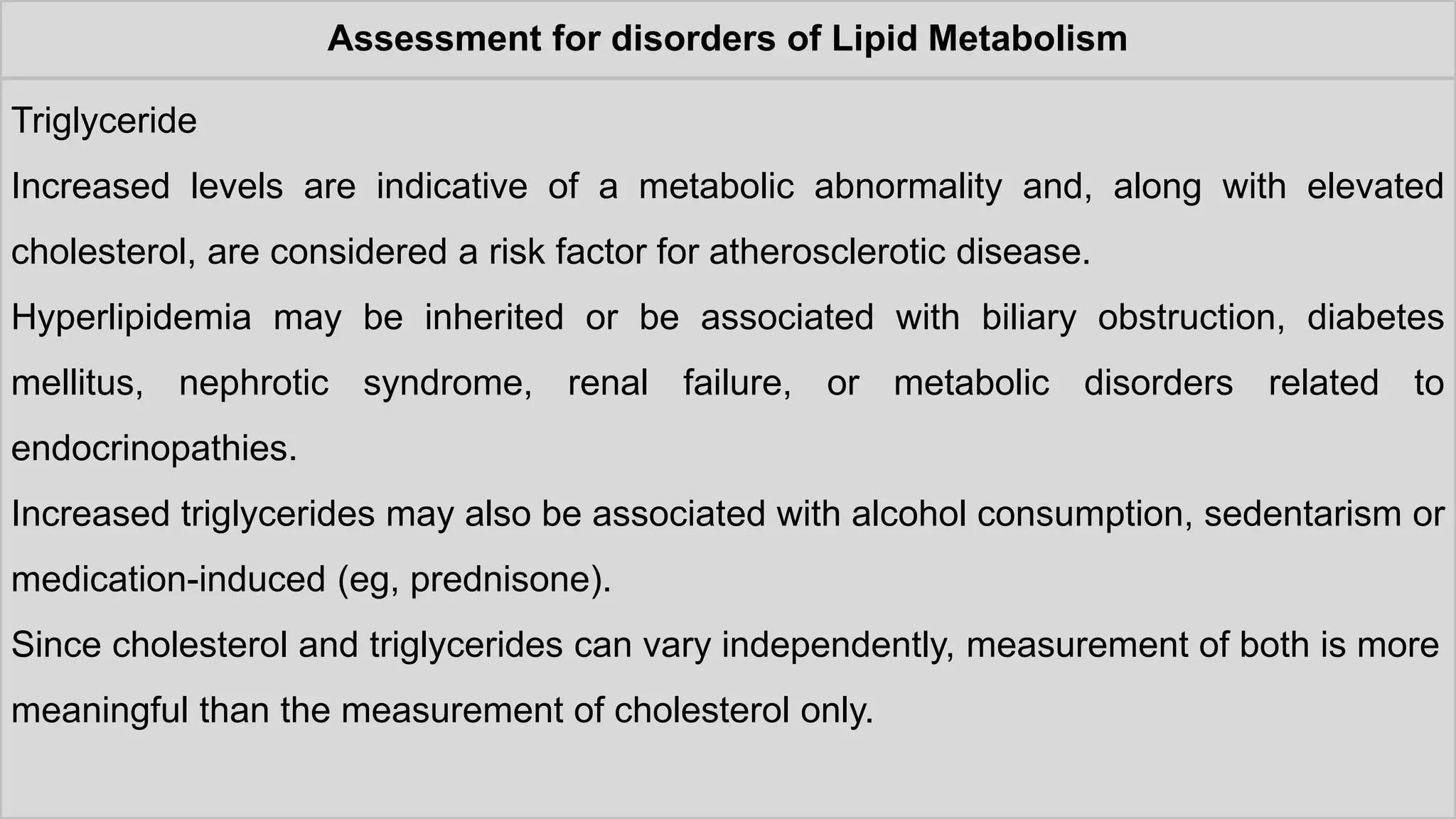
Assessment for disordersof Lipid Metabolism
Triglyceride
Increased levels are indicative of a metabolic abnormality and, along with elevated
cholesterol, are considered a risk factor for atherosclerotic disease.
Hyperlipidemia may be inherited or be associated with biliary obstruction, diabetes
mellitus, nephrotic syndrome, renal failure, or metabolic disorders related to
endocrinopathies.
Increased triglycerides may also be associated with alcohol consumption, sedentarism or
medication-induced (eg, prednisone).
Since cholesterol and triglycerides can vary independently, measurement of both is more
meaningful than the measurement of cholesterol only.
35.
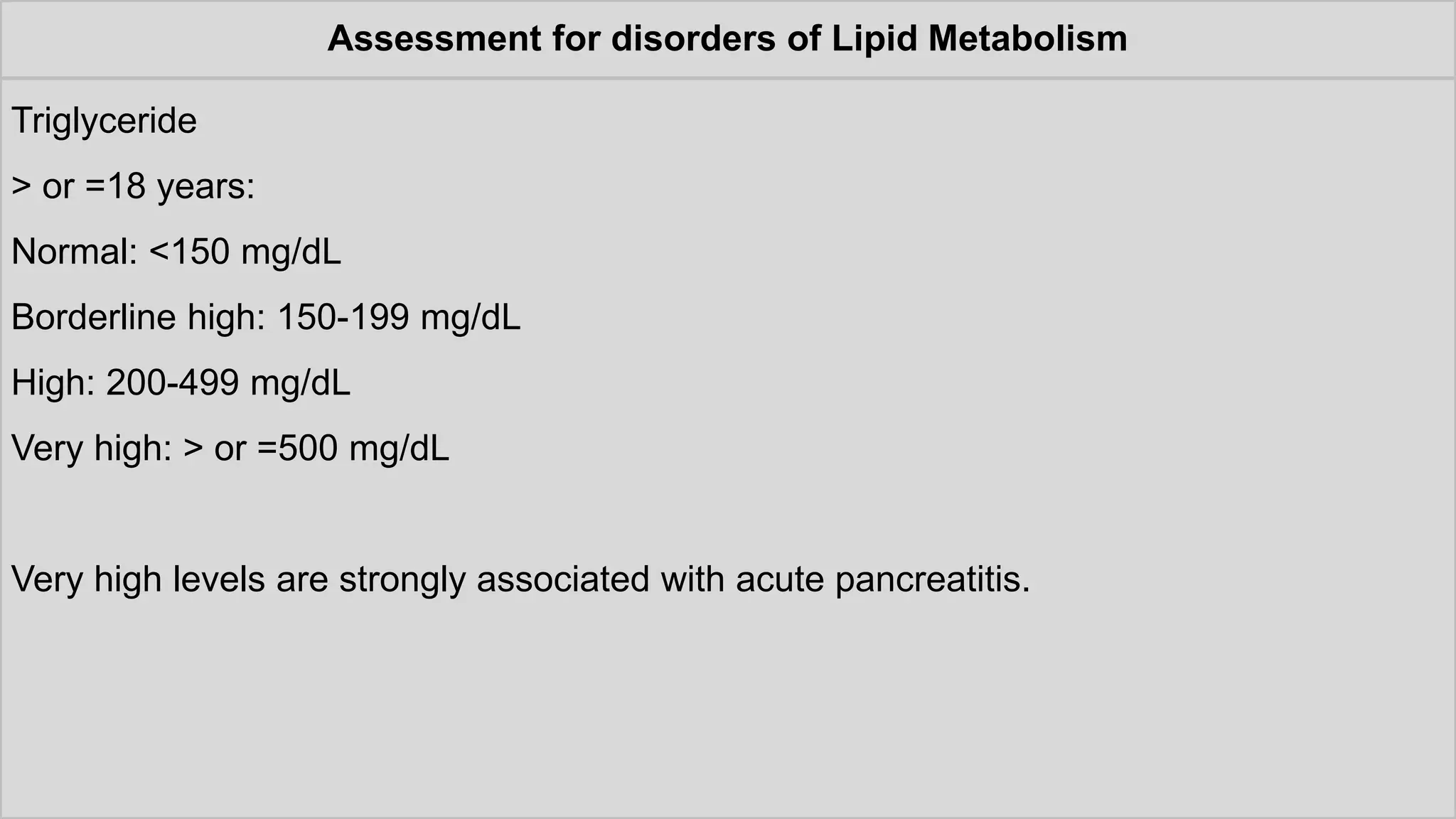
Assessment for disordersof Lipid Metabolism
Triglyceride
> or =18 years:
Normal: <150 mg/dL
Borderline high: 150-199 mg/dL
High: 200-499 mg/dL
Very high: > or =500 mg/dL
Very high levels are strongly associated with acute pancreatitis.
![Assessment for disorders of Lipid Metabolism
Friedewald Formula
• LDL-C = TC – (TG/5 + HDL-C) [mg/dL]
• Requirements
• Triglyceride to Cholesterol ratio in Very Low Density Lipoprotein (VLDL) is relatively
constant in normal subjects and nearly all patients with dyslipidemia at about 5:1
• When chylomicrons are not detectable in the blood, most of the triglyceride in
plasma is from VLDL (Fasting – 12 hours)
• Not accurate when TG is greater than 400mg/dL
• Not reliable when LDL-C is less than 70mg/dL](https://image.slidesharecdn.com/1lipidsandlipoproteins20241-251123101304-05e5dbc3/75/1-Lipids-and-Lipoproteins-2024gb-1-pdf-15-2048.jpg)
![Assessment for disorders of Lipid Metabolism
Plasma Apolipoprotein B
• present on atherogenic lipoproteins and serves as a macromolecular scaffold to
provide structural integrity. I
• t also serves as a ligand for the LDL receptor, which facilitates its clearance from the
plasma.
• There are two major isoforms of apoB: apoB48, found on intestinally derived
lipoproteins (chylomicrons and their remnants) and apoB100, found on hepatically
derived lipoproteins – very LDL, intermediate-density lipoprotein, LDL and lipoprotein
(a) (Lp[a]).
.](https://image.slidesharecdn.com/1lipidsandlipoproteins20241-251123101304-05e5dbc3/75/1-Lipids-and-Lipoproteins-2024gb-1-pdf-18-2048.jpg)




















![Lipoprotein metabolism and CAD[1].pptx..](https://cdn.slidesharecdn.com/ss_thumbnails/lipoproteinmetabolismandcad1-250223181828-e4e0a658-thumbnail.jpg?width=640&height=640&fit=bounds)



























