Downloaded 76 times
![Mental illness /Disorder
Mental illness /Disorder
Mental disorder is “a clinically significant
behavioural or psychological syndrome or
pattern that occurs in an individual and that is
associated with distress or disability or with a
significantly increased risk of suffering death,
pain, disability, or an important loss of
freedom”
(American Psychological Association [APA])](https://image.slidesharecdn.com/principlesandconceptsinmentalhealthnursing-241214185236-e2751434/75/principles-and-concepts-in-Mental-health-nursing-ppt-7-2048.jpg)






![NURSING IN
NURSING IN
SECONDARY
SECONDARY PREVENTION
PREVENTION
• Ongoing assessment of individuals at high risk for illness
exacerbation (e.g., during home visits, at day care, in
community health centers, or in any setting where screening
of high-risk individuals might occur).
• Provision of care for individuals in whom illness symptoms
have been assessed (e.g., individual or group counseling,
medication administration, education and support during
period of increased stress [crisis intervention], staffing rape
crisis centers, suicide hotlines, homeless shelters, shelters for
abused women, or mobile mental health units).](https://image.slidesharecdn.com/principlesandconceptsinmentalhealthnursing-241214185236-e2751434/75/principles-and-concepts-in-Mental-health-nursing-ppt-136-2048.jpg)


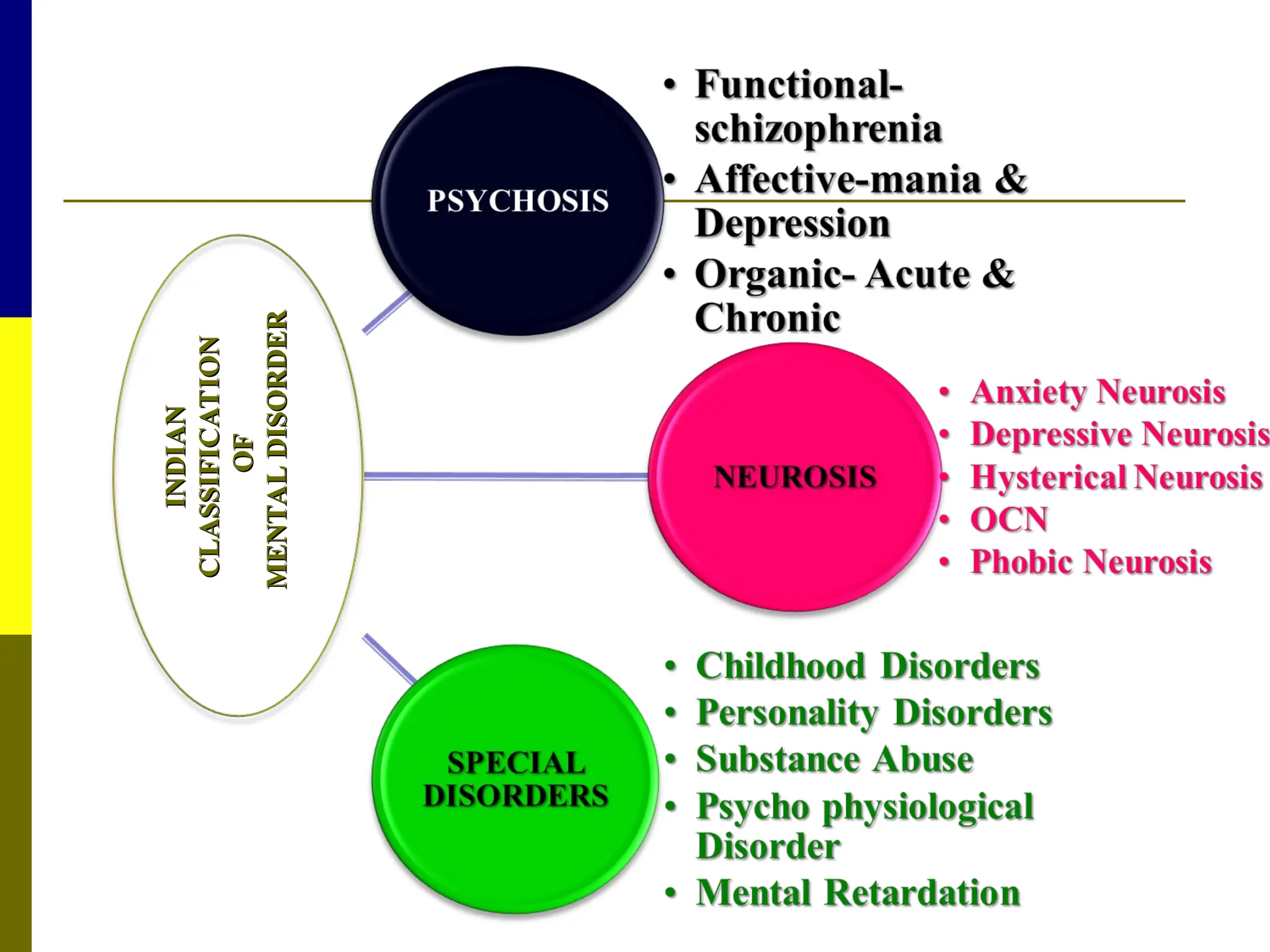
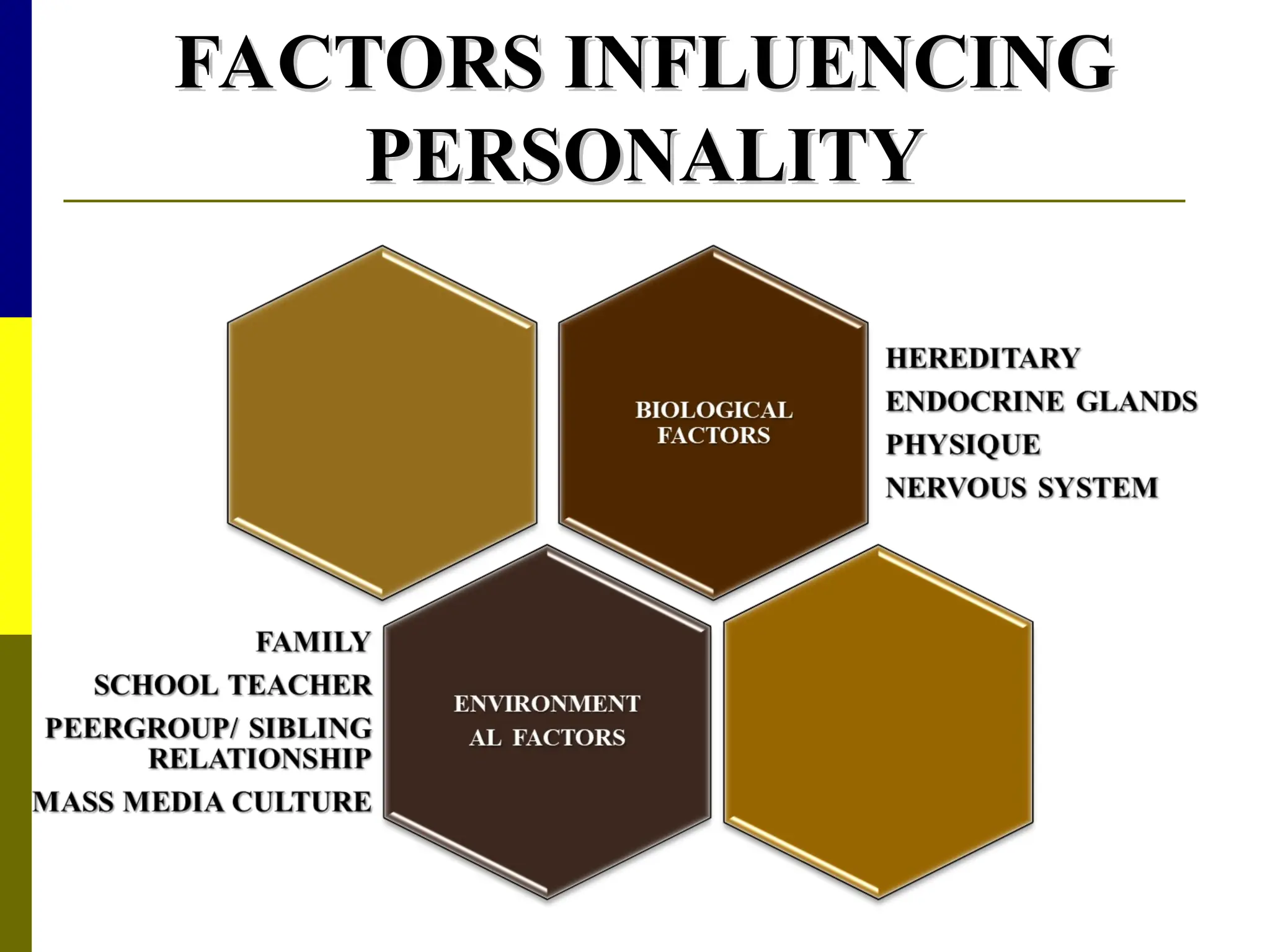
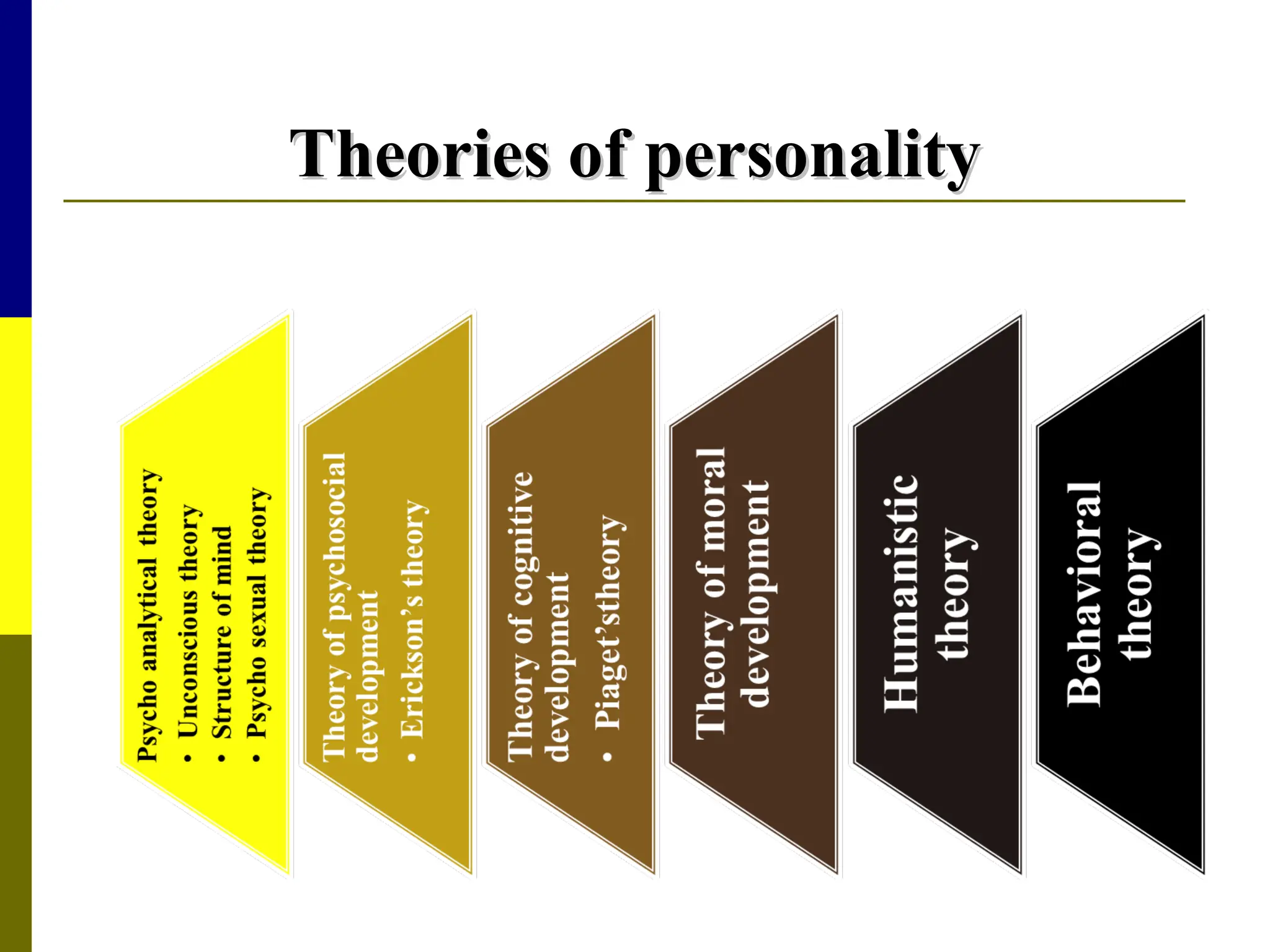
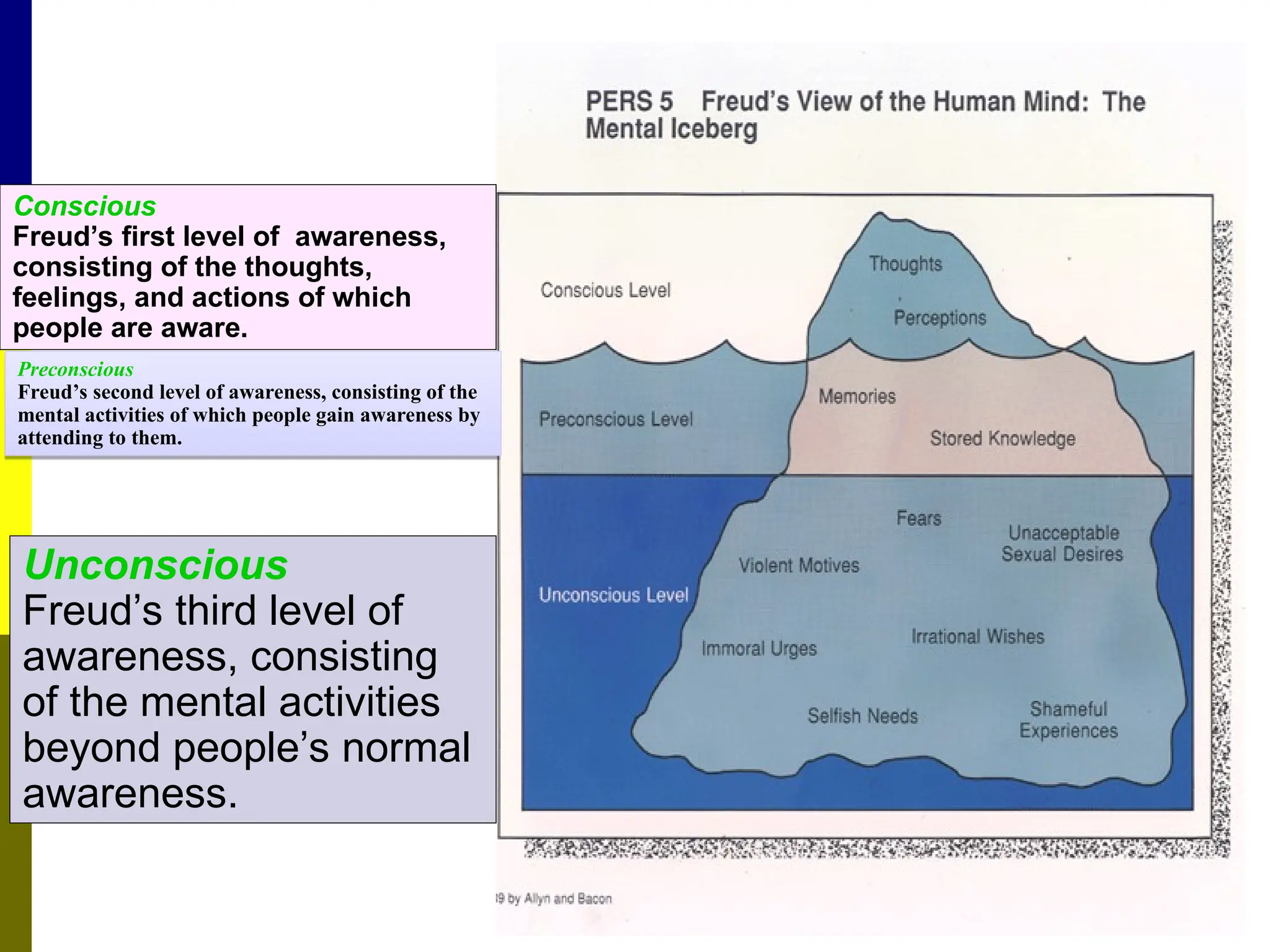
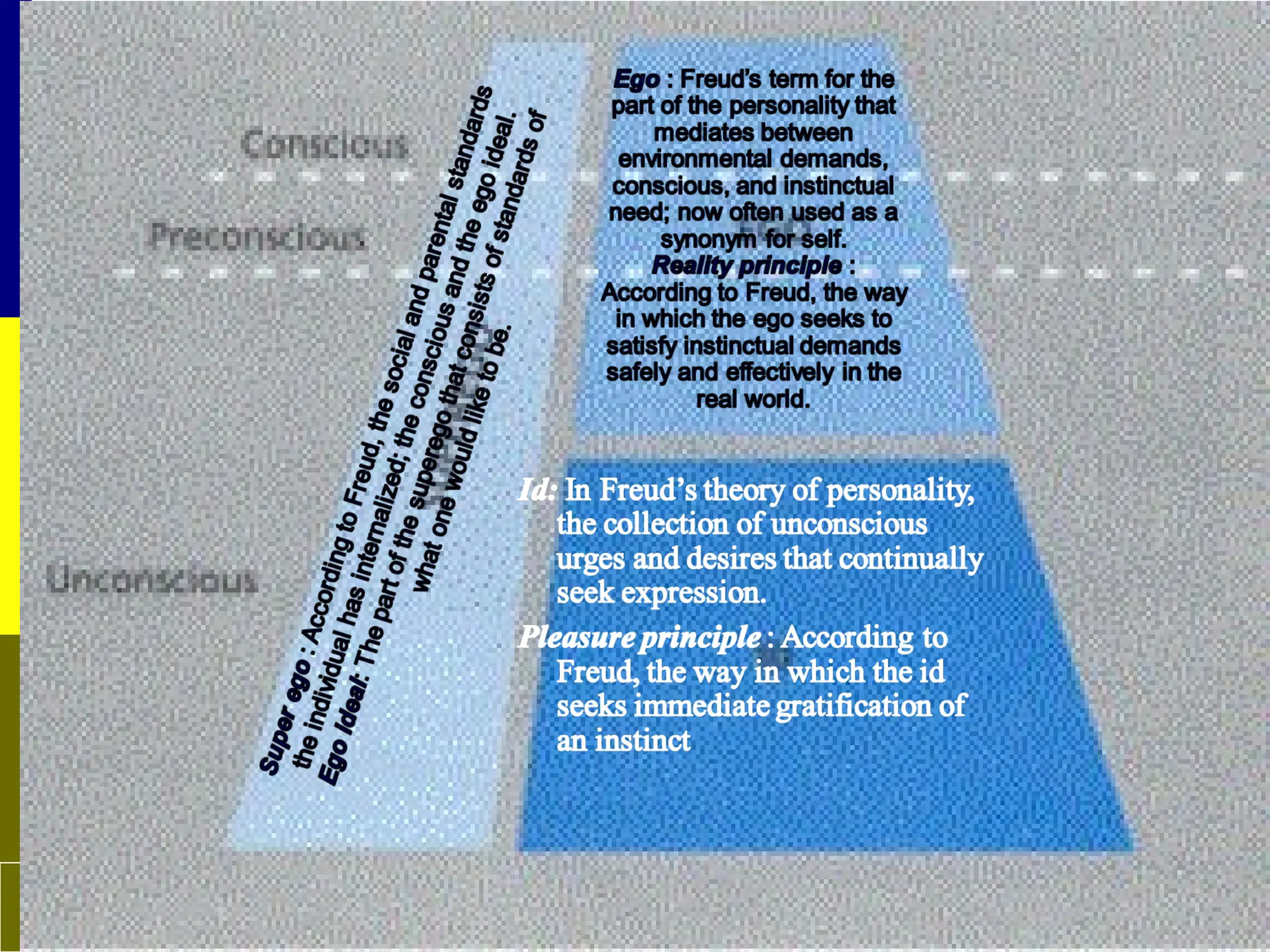
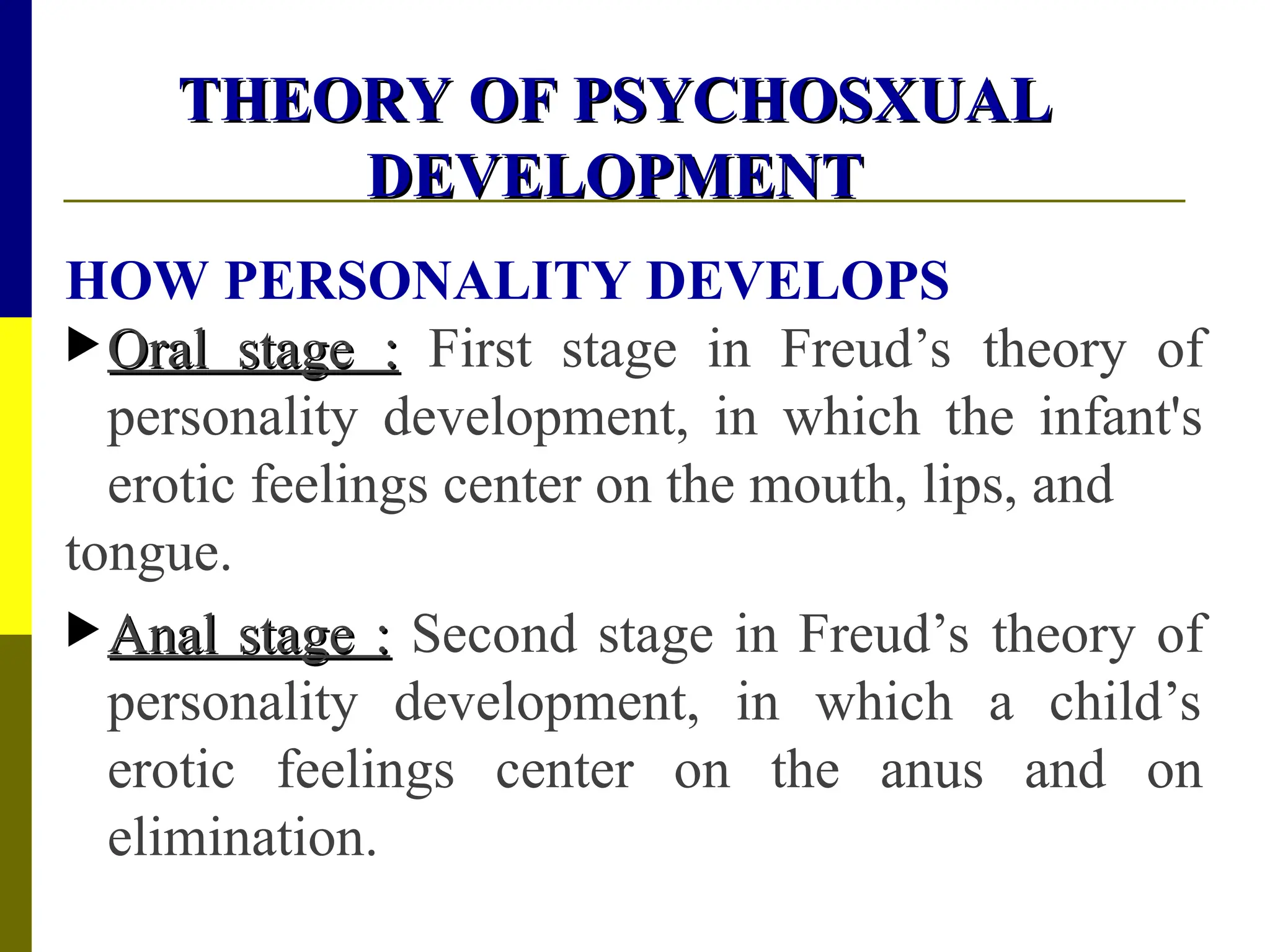
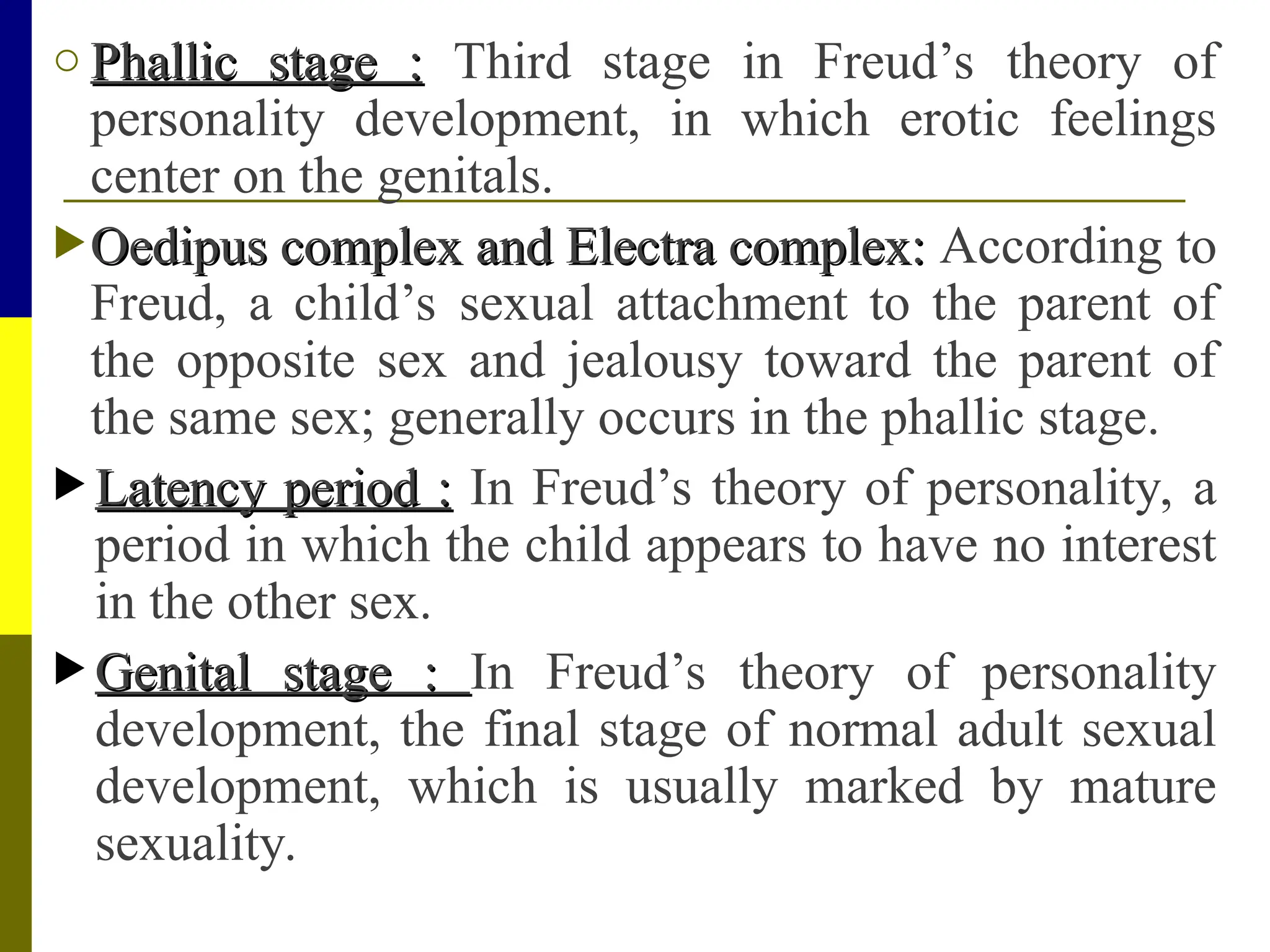
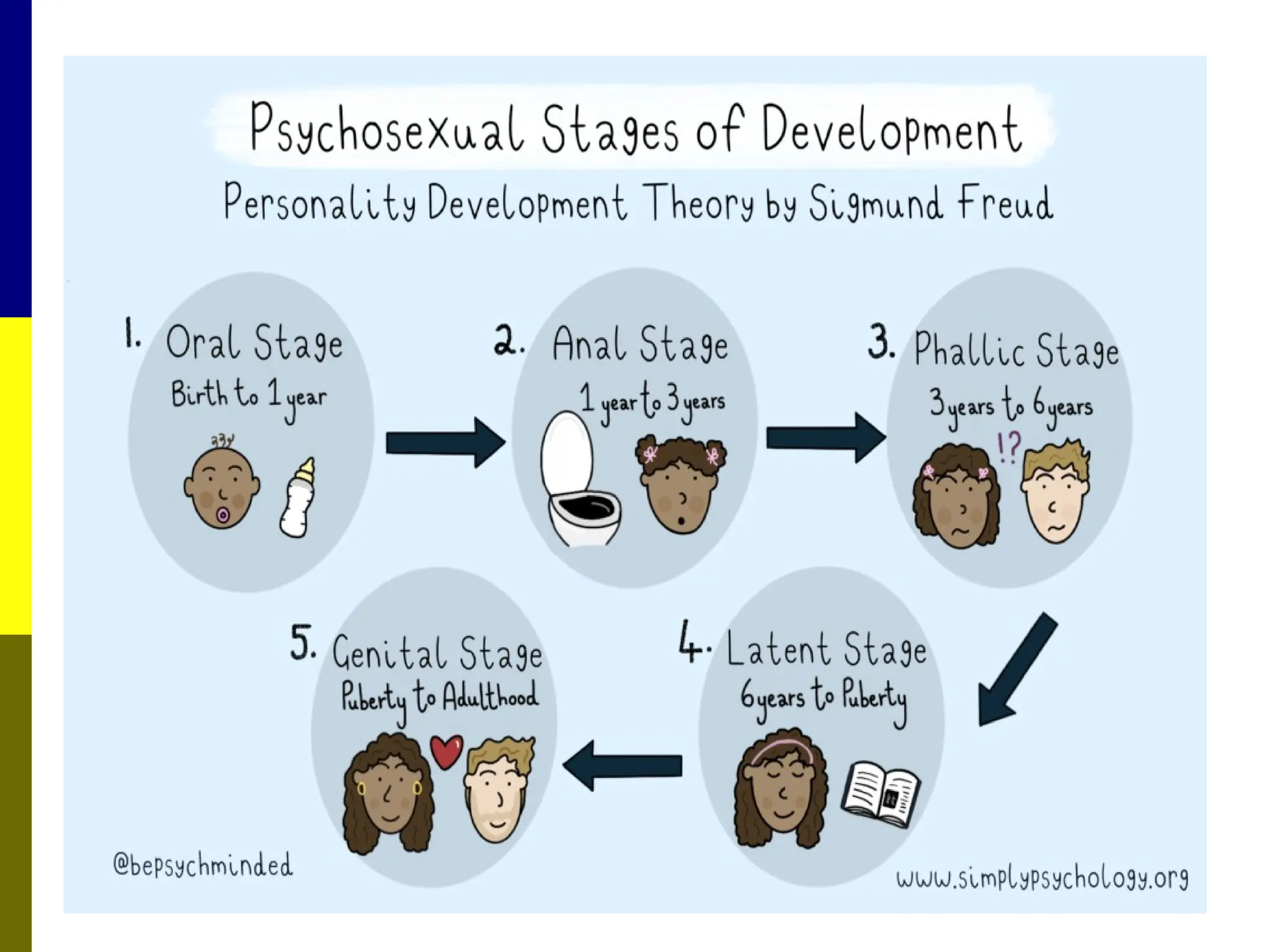
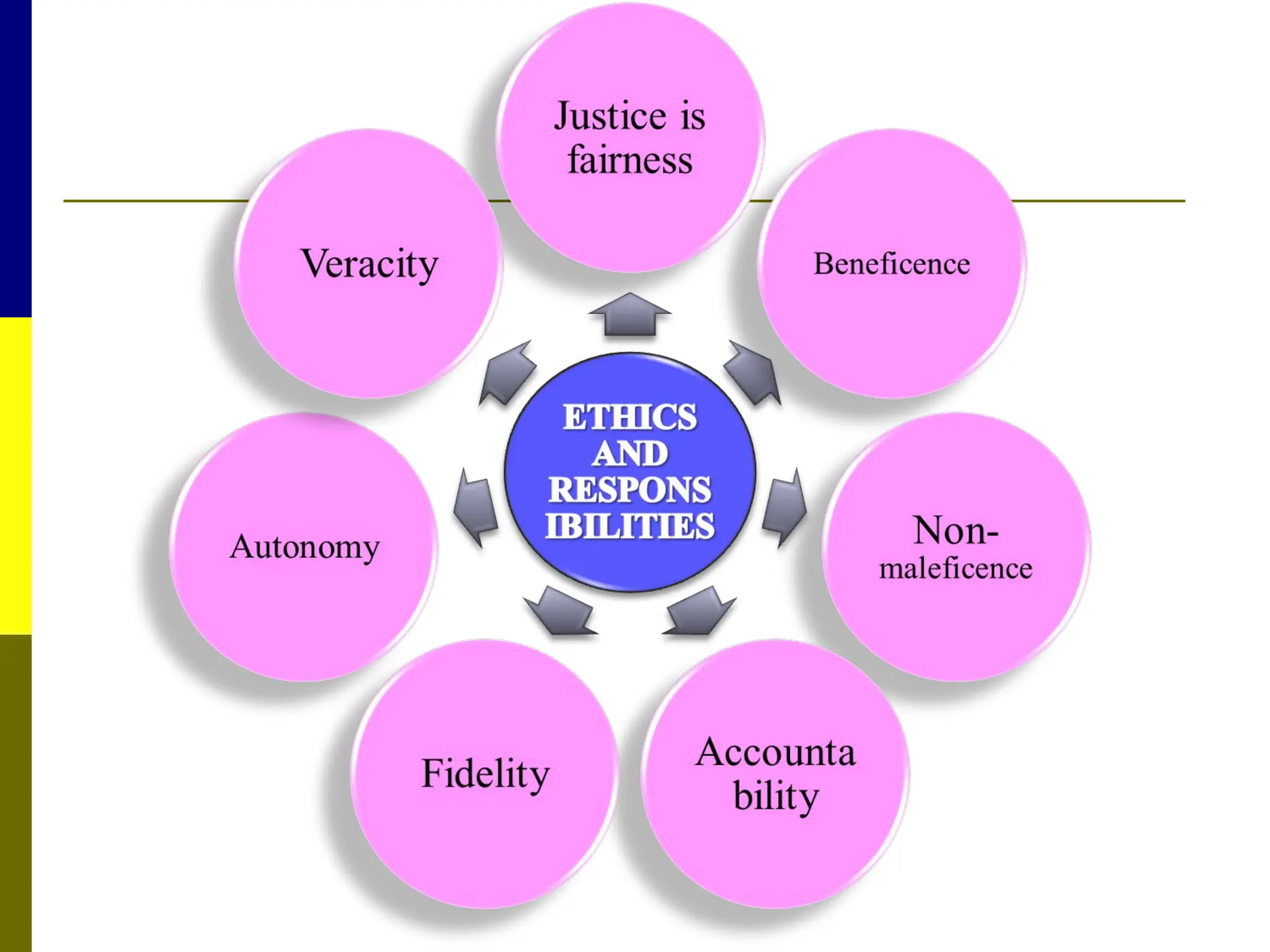
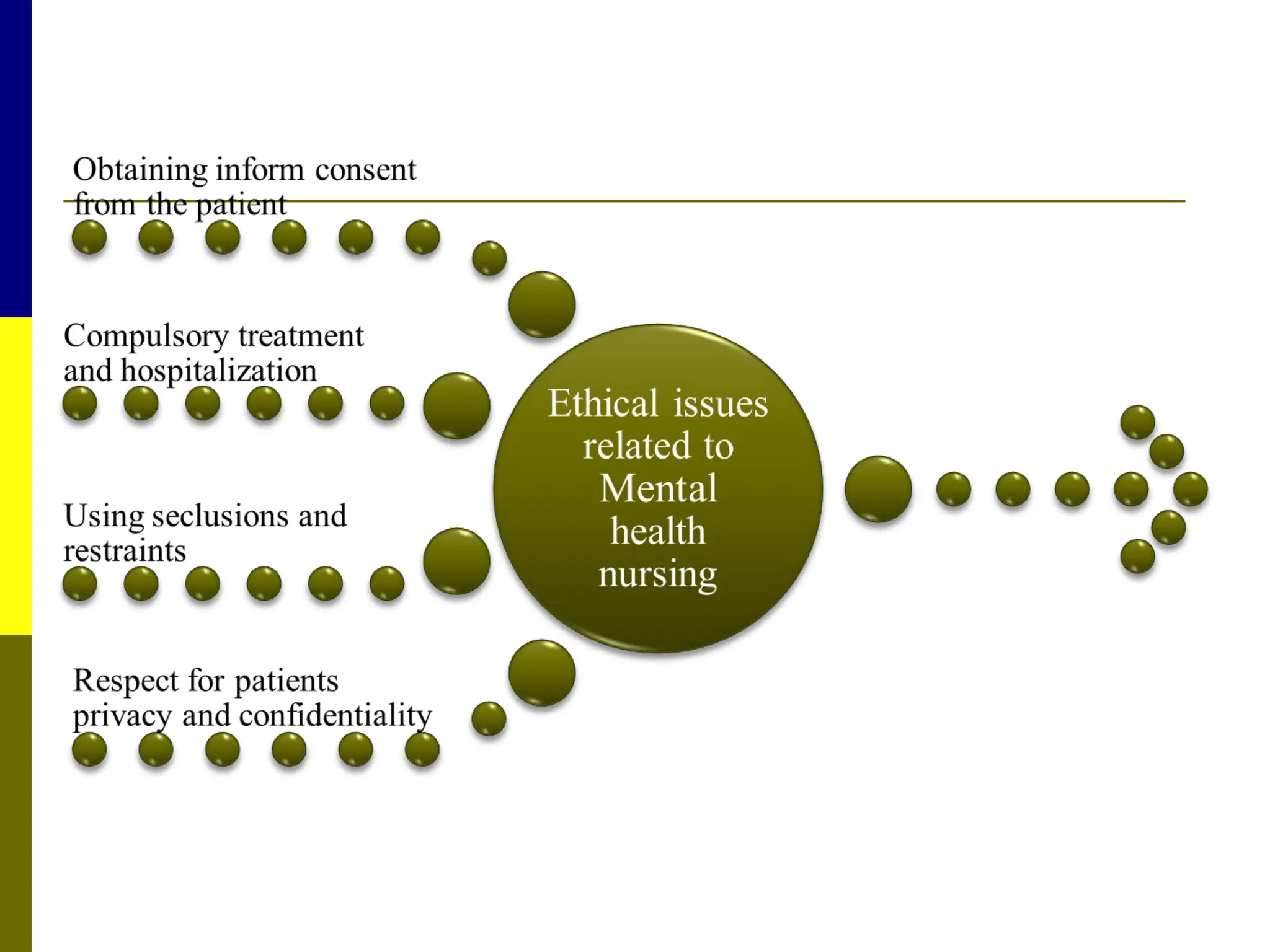
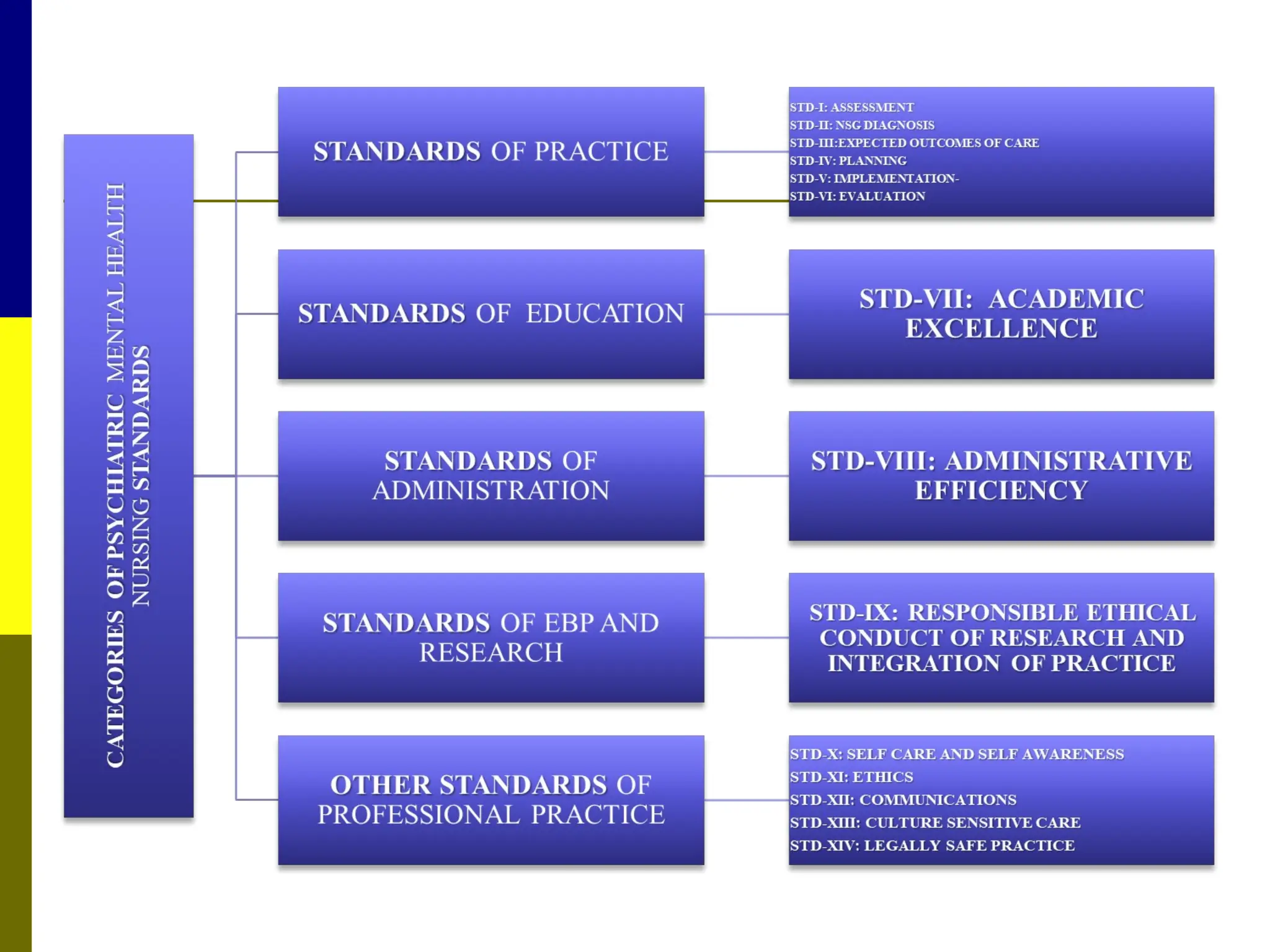
The document provides a comprehensive overview of mental health nursing, covering definitions, classifications of mental disorders, and principles of psychiatric nursing. It discusses various models of mental health, the etiology of mental disorders, psychopathology, and key concepts such as personality development, compulsions, delusions, and classifications within psychiatric practice. Additionally, it highlights ethical responsibilities and practice standards in mental health nursing, alongside details on geriatric psychiatry and personality theories.
































![PRESENTATION ON MHN UNIT 2 PPTX[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonmhnunit2pptx1-250906125029-cec4c130-thumbnail.jpg?width=640&height=640&fit=bounds)


![2._Psychopathology,_ET[1] psychiatry courses.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/2-241125165215-eb011694-thumbnail.jpg?width=640&height=640&fit=bounds)


![MENTAL STATUS EAMINATION[MSE] for undergraduates (Psych)](https://cdn.slidesharecdn.com/ss_thumbnails/mentalstatuseaminationmseforundergraduatespsych-250812021929-dd507eb8-thumbnail.jpg?width=640&height=640&fit=bounds)





![SYMPTOMATOLOGY group 1 and 2 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/symptomatologygroup1and2autosaved-250615072117-505e8c1d-thumbnail.jpg?width=640&height=640&fit=bounds)










































