The document discusses the legal aspects of psychiatric nursing, including key legal issues, types of laws, and the rights of mentally ill patients in India, with an emphasis on the evolution of psychiatric care and relevant legislation like the Mental Health Act. It highlights the responsibilities of psychiatric nurses in relation to legal standards, ethical principles, and patient advocacy, while also addressing common legal challenges such as consent, confidentiality, and the use of restraints. Furthermore, it reflects on the importance of understanding these legal obligations to improve nursing practices and protect patient rights.
Introduces legal issues in psychiatry nursing, overview objectives, types, and rights of the mentally ill.
Discusses the evolution and importance of legal issues in psychiatry nursing and the nurse's accountability.
Outlines the objectives of laws protecting public rights, introducing types of laws relevant to nursing.
Focuses on confidentiality, patient privacy, consent, and the ethical dimensions nurses must uphold.
Explains informed consent, its elements, types of consent, highlighting patient autonomy.
Defines restraints and guidelines for their use, emphasizing patient dignity and safety.
Describes seclusion practices and legal implications of false imprisonment in psychiatric settings.
Covers various torts relevant to nursing, including negligence and malpractice.
Presents research findings on staff nurses' knowledge of legal aspects before and after training.
Highlights the development of psychiatry in India and key features of the Mental Health Act.
Details on the structure, admission processes, and contents of the Mental Health Act 1987.
Discusses the key features and changes introduced by the Mental Healthcare Act of 2017. Reviews provisions for advance directives, consent, and legal support for mental health patients.Summarizes rights granted to individuals under the Mental Healthcare Act 2017.
Discusses the relationship between psychiatry and law, competencies in treatment, and assessments.
Analyzes the knowledge gaps among psychiatric nurses and emphasizes the importance of understanding legalities.Concludes that psychiatric nurses must be aware of legal issues to protect themselves and advocate for clients.Provides sources and references used within the presentation related to legal aspects in psychiatric nursing.
LEGAL ASPECTS OF
PSYCHIATRYNURSING
MODERATOR
AJESH KUMAR T.K.
ASSOCIATE PROFESSOR
CON AIIMS NEW DELHI
PRESENTER
VASHU CHAUHAN
MSC NURSING 1ST
YEAR
CON AIIMS NEW DELHI
2.
What arelegal issues, their
objectives and types
Legal issues in psychiatry
nursing
Lawsuits in psychiatry
nursing
Development of psychiatry
in India
Rights of mentally ill and
role of nurses in the care
Forensic psychiatry
3.
INTRODUCTION
• The practiceof psychiatric nursing has changed immensely in recent
decades. Advances in understanding of mental illness and innovations
in treatment, societal forces, economic restrictions and informed
patients and families have promoted the changes.
• With the clinical evolution of psychiatric care, the definition of legal
practice also has evolved over time. Psychiatric nurses are held
accountable to practice according to current laws and standards.
4.
WHAT IS ALEGAL ISSUE?
• ‟Legal issues are those that are decided by
law″
• In Psychiatry legal issues is a subject of
intricacies and require the nurses to be well
versed with the laws in order to both guide
her practice and encourage advocacy.
5.
OBJECTIVES OF LAWS
1.Intended to protect the rights of the public.
2. Nurses familiarity with the laws enhances their ability to be client
advocates.
3. Laws assist in the decision-making process involved in nursing
practice.
4. The ultimate goal of all laws is to promote peaceful and productive
interaction among the people of that society.
CIVIL LAW
• Dealswith disputes between individuals,
organizations, private rights.
• Primarily focused on providing relief and
compensation to victims.
EXAMPLES
1. Contract disputes
2. Property disputes
3. Family disputes [Divorce]
8.
CRIMINAL LAW
• Involvesoffences against state or
public.
• Prevent harmful actions and punish
offenders violating law and order.
EXAMPLES
1) Murder
2) Theft
3) Assault
9.
DIFFERENCE
• Civil vs.Criminal Law: Civil law
addresses private disputes
between individuals or entities,
while criminal law deals with
offenses against society as a
whole.
10.
COMMON LAW
• Commonlaw is a body of law that is
developed through court decisions
rather than through written statutes.
• It evolves based on judicial rulings
and interpretations.
• Judge-made these laws and
developed over time through
decisions in individual court cases.
11.
Statutory law consistsof
written laws passed by
legislative bodies such as
congress or Parliament. These
are formal statutes that specify
what is legal or illegal,
outlining the rights and duties
of individuals.
• Examples: Traffic laws, tax
laws, environmental
regulations, labor laws.
12.
DIFFERENCE
• Statutory vs.Common Law:
Statutory law is written and
enacted by legislatures, while
common law is based on
judicial precedents and past
rulings.
13.
LEGAL ISSUES INPSYCHIATRY
NURSING
Confidentiality And Right To Privacy
Consent
Restraints And Seclusion
False Imprisonment
14.
CONFIDENTIALITY
• Confidentiality inpsychiatry is a
fundamental ethical and legal principle
that ensures patient information is
protected and only shared with
authorized individuals.
• It Is crucial in establishing trust
between psychiatric patients and
healthcare providers.
15.
KEY ASPECTS
1. Protectionof Patient information
2. Breaches in Special Situations
3. Sharing Information with Other Healthcare Providers
4. Minors and confidentiality
5. Confidentiality in Group Therapy
16.
RIGHT TO PRIVACY
•The right to privacy in psychiatry is a crucial legal and ethical principle
that protects a patient’s personal and mental health information from
bring disclosed.
• highly significant in psychiatry where patients often reveal deeply
personal and sensitive information as part of their treatment and
should be prevented from being disclosed without their consent.
18.
CONSENT
• Informed consentin psychiatry is the process by which a patient
voluntarily agrees to receive mental health treatment after being fully
informed about the nature, risks, benefits, and alternatives of the
proposed treatment.
• According to law, all individuals have the right to decide whether to
accept or reject treatment.
19.
• The rationalefor the
doctrine of informed
consent is the preservation
and protection of Individual
autonomy in determining
what will and will not
happen to the person’s body
(Guido, 2006)
20.
ELEMENTS OF INFORMED
CONSENT
•KNOWLEDGE
• COMPETENCY
• FREE WILL
The following
three major
elements of
informed
consent must
been
addressed
21.
TYPES OF CONSENT
•There are two types of consent we use in case of psychiatry
• providing an individual with relevant
information about a procedure or
treatment before obtaining their
permission to proceed.
INFORMED
CONSENT
• usually a legal representative of an
individual who is incapable of giving
informed consent.
SUBSTITUED
CONSENT
22.
RESTRAINTS
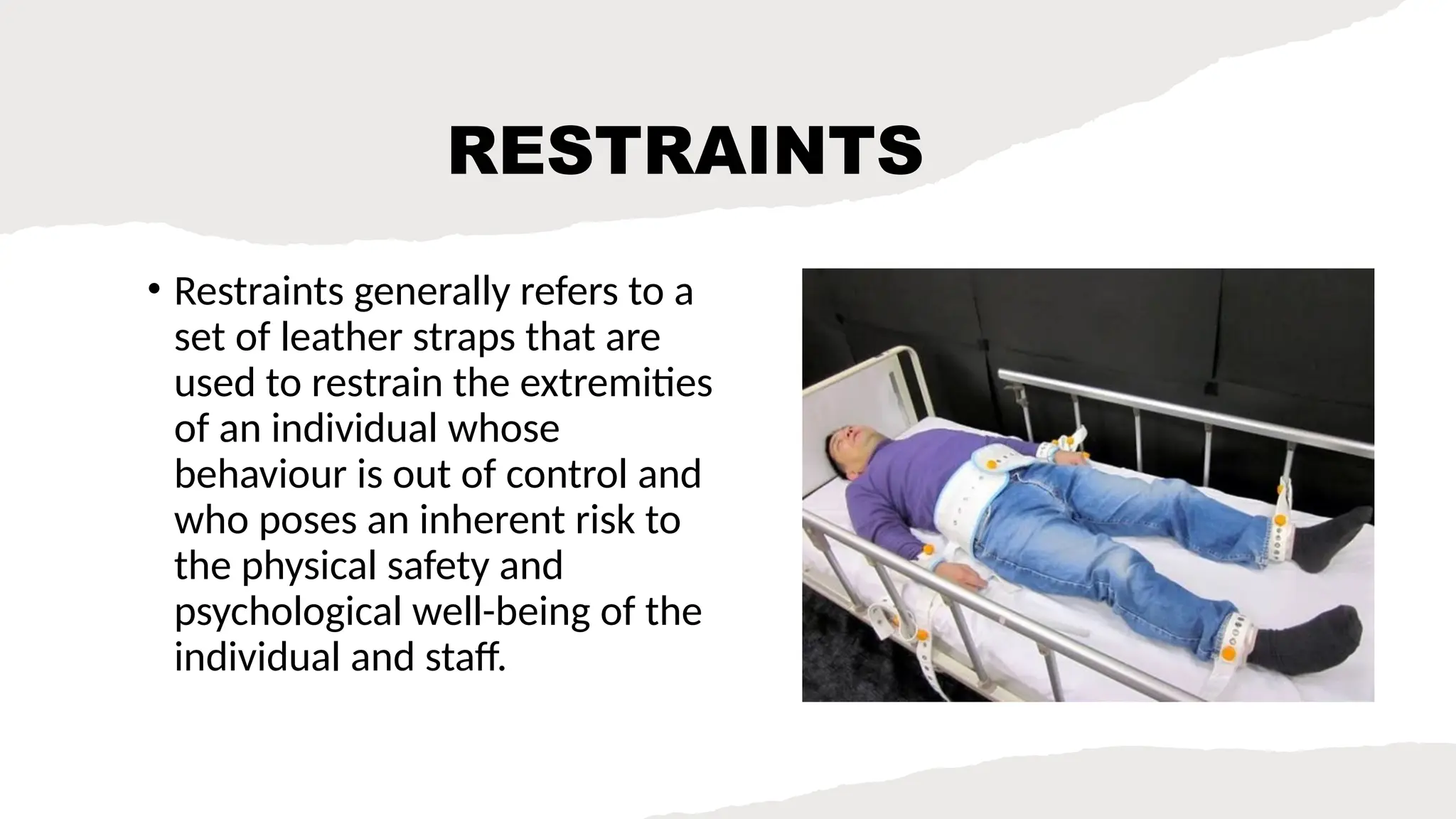
• Restraints generallyrefers to a
set of leather straps that are
used to restrain the extremities
of an individual whose
behaviour is out of control and
who poses an inherent risk to
the physical safety and
psychological well-being of the
individual and staff.
23.
REMEMBER..
1. Never tobe used as a way of punishment to patient.
2. Should not be used according to staff convenience.
3. Written consent must be taken except in cases of emergency
when patient is dangerous for self or for others.
4. the use of mechanical restraints is for 1 hour and in adults, for
4 hours only during which the limb assessment is to be done
every 15 minutes.
5. Verbal interventions and chemical restraints are prioritized
before physical restraints.
24.
SECLUSIONS
• It isanother type of physical
restraint in which the client is
confined alone in a room from
which he or she is unable to
leave. The room is usually
minimally furnished with items
to promote the client’s comfort
and safety.
25.
FALSE IMPRISONMENT
• Itis the deliberate and unauthorized
confinement of a person within fixed
limits by the use of verbal or physical
means.
• Healthcare workers may be charged
with false imprisonment for restraining
or Secluding against the wishes of the
client anyone having been admitted to
the hospital Voluntarily.
26.
TORTS
• "A civilwrong
committed against a
person or person’s
property″
Contd..
• Negligence -Misconductor practice that is below the standard
expected of an ordinary, reasonable and prudent person which places
another person at risk for harm
• Malpractice - occurs when a nurse fails to provide the standard of
care expected, resulting in harm or injury to a patient
29.
Contd..
• Assault- Refersto the intentional act of threatening or
attempting to cause harm to a patient, without their consent,
which creates a reasonable fear of imminent harm
• Battery - occurs when a nurse intentionally touches or performs
a procedure on a patient without their consent, leading to an
unwanted or offensive physical contact. Unlike assault, which
involves the fear of harm, battery involves actual physical
contact, regardless of whether it causes injury.
30.
• Invasion ofprivacy : refers to the improper handling or disclosure of a
patient’s personal and medical information, or intrusion into a patient’s
private life without consent.
• Misdemeanors : typically involve minor crimes or misconduct and carry
less severe penalties
• felony : it is a serious crime that is more severe than a misdemeanor,
often punishable by imprisonment for more than one year,
• Defamation : it is the act of making false statements about someone that
harm their reputation. Defamation can occur in two forms:
1. Libel: Defamation in written or published form (e.g., newspapers, online
articles, social media posts).
2. Slander: Defamation through spoken statements (e.g., conversations,
speeches, broadcasts).
31.
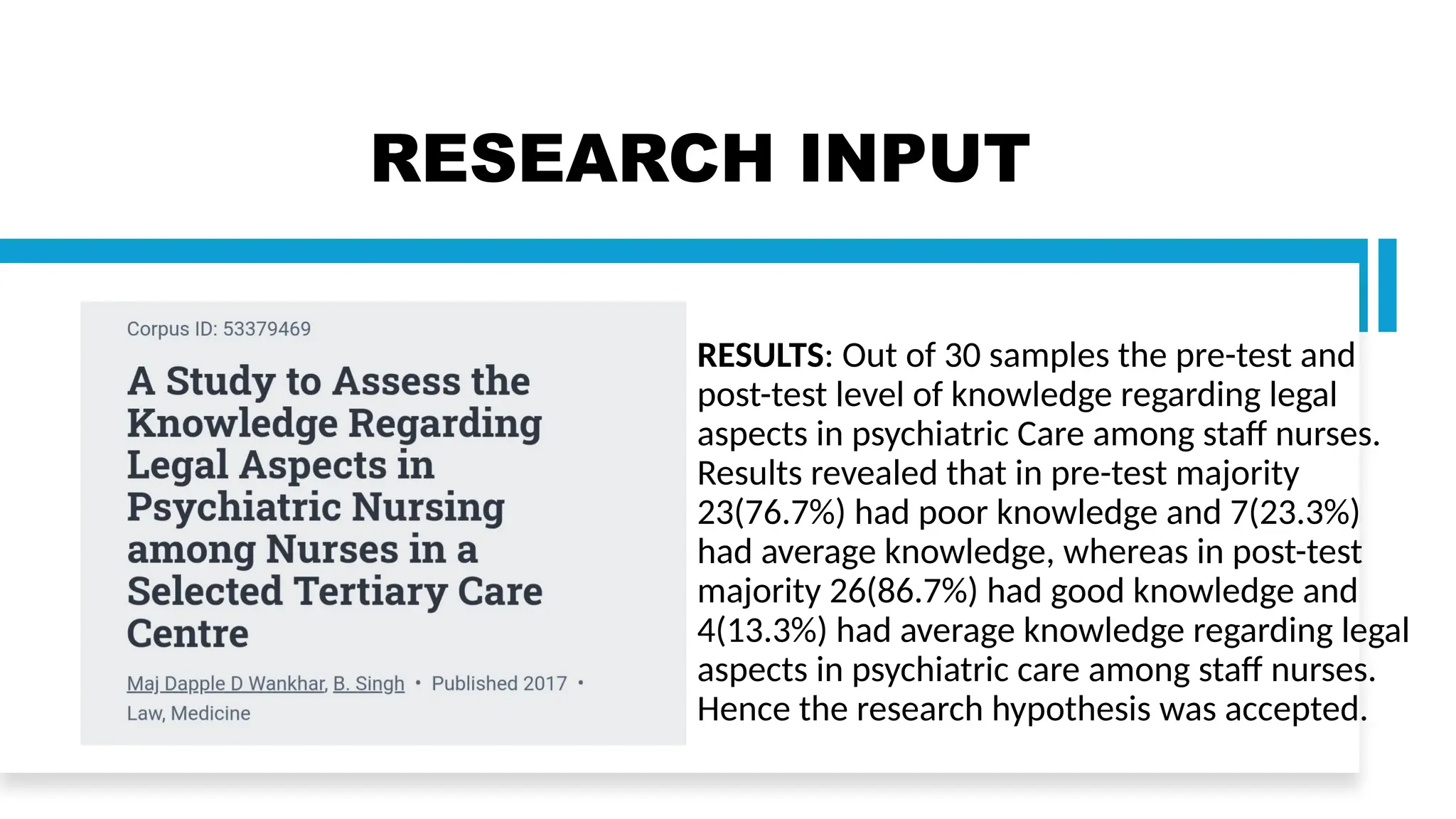
RESEARCH INPUT
RESULTS: Outof 30 samples the pre-test and
post-test level of knowledge regarding legal
aspects in psychiatric Care among staff nurses.
Results revealed that in pre-test majority
23(76.7%) had poor knowledge and 7(23.3%)
had average knowledge, whereas in post-test
majority 26(86.7%) had good knowledge and
4(13.3%) had average knowledge regarding legal
aspects in psychiatric care among staff nurses.
Hence the research hypothesis was accepted.
32.
PSYCHIATRY
IN INDIA
• Psychiatryin India has
evolved significantly over
the years, addressing a
range of mental health
issues influenced by
cultural, social, and
economic factors. Here’s
an overview of the current
landscape
33.
MENTAL
HEALTH ACT
1987
• IndianMental Health Act
was drafted by the
parliament in 1987 but it
came into effect in all the
States and union territories
of India in April 1993.
• This act replaced the Indian
lunacy act of 1912.
34.
AIMS
1. To Changethe attitudes of the society towards the mentally ill and
considerably realised that no stigma should be attached to such
illness.
2. Modify the act according to the rapid advancement of medical
science .
3. Regulate the power of the government for establishing licensing
and controlling psychiatric hospitals and psychiatric homes.
35.
Contd..
4. Provide legalaid to mentally ill persons and to protect them from
being detained in psychiatric hospitals without sufficient evidence
of their illness.
5. Building regulating and maintaining central and state authorities for
mental health services.
36.
CHAPTERS
• CHAPTER 1– PRELIMINARY INFORMATION
1-Psychiatric hospital / nursing home -It is an established or maintained
unit by the government or by any other person for the care of mentally ill
persons.
2-Mentally ill person- a person who is in need of treatment by reason of
any mental disorder other than mental retardation.
3-Psychiatrist - medical practitioner possessing post graduation degree or
diploma in psychiatry recognised by the Medical Council of India.
37.
• CHAPTER 2-it deals with establishment of central and state authorities
for regulation and coordination of mental health services.
• CHAPTER 3 - it provides guidelines for establishment and maintenance
of psychiatric hospitals and nursing homes
• CHAPTER 4- it deals with the procedure for admission and detention in
psychiatry unit as the admission process varies differently in different
cases for the psychiatric unit.
38.
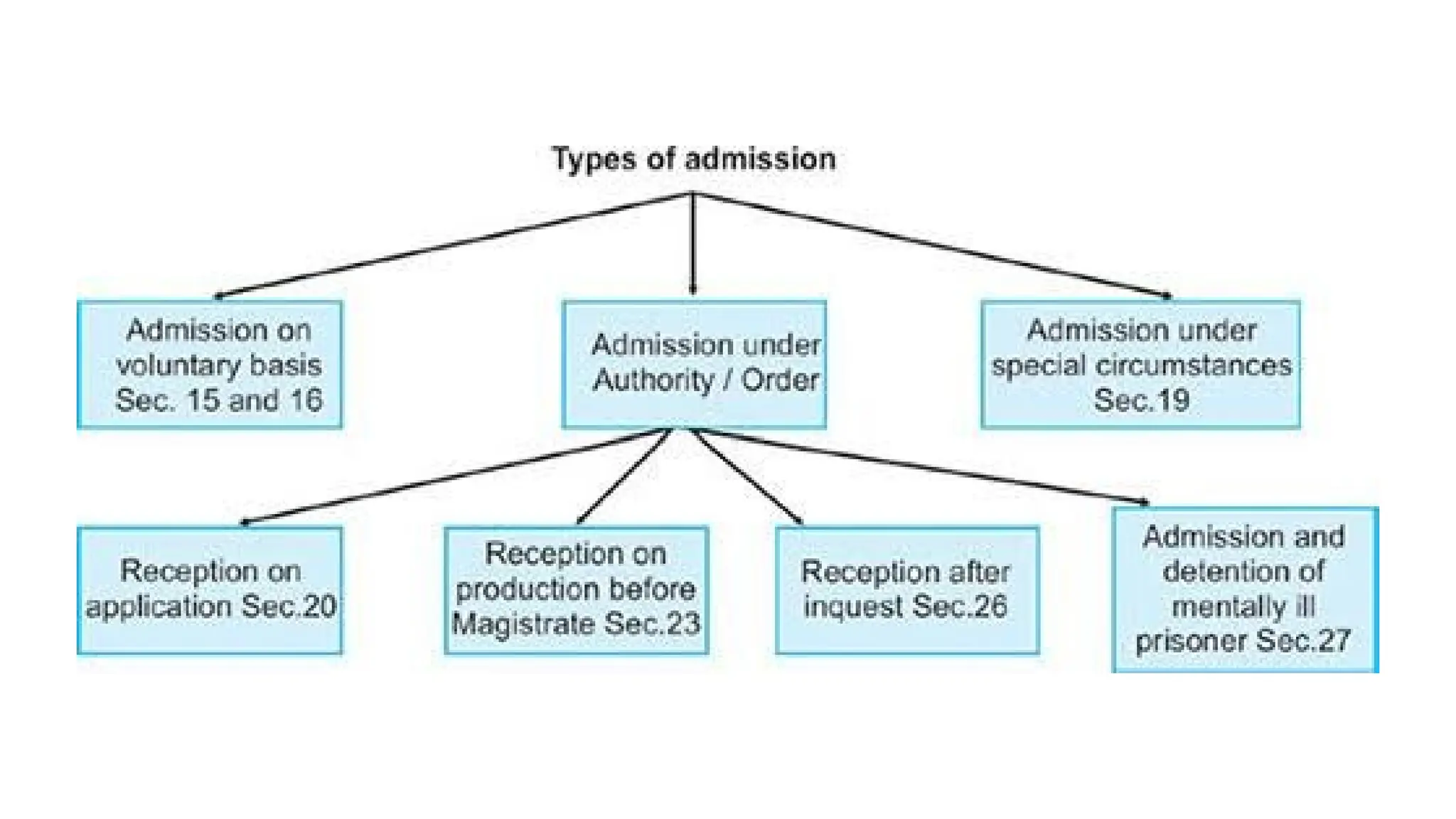
TYPES OF ADMISSION
ADMISSIONON VOLUNTARY BASIS
ADMISSSION ON SPECIAL
CIRCUMSTANCES
ADMISSION UNDER RECEPTION ORDER
43.
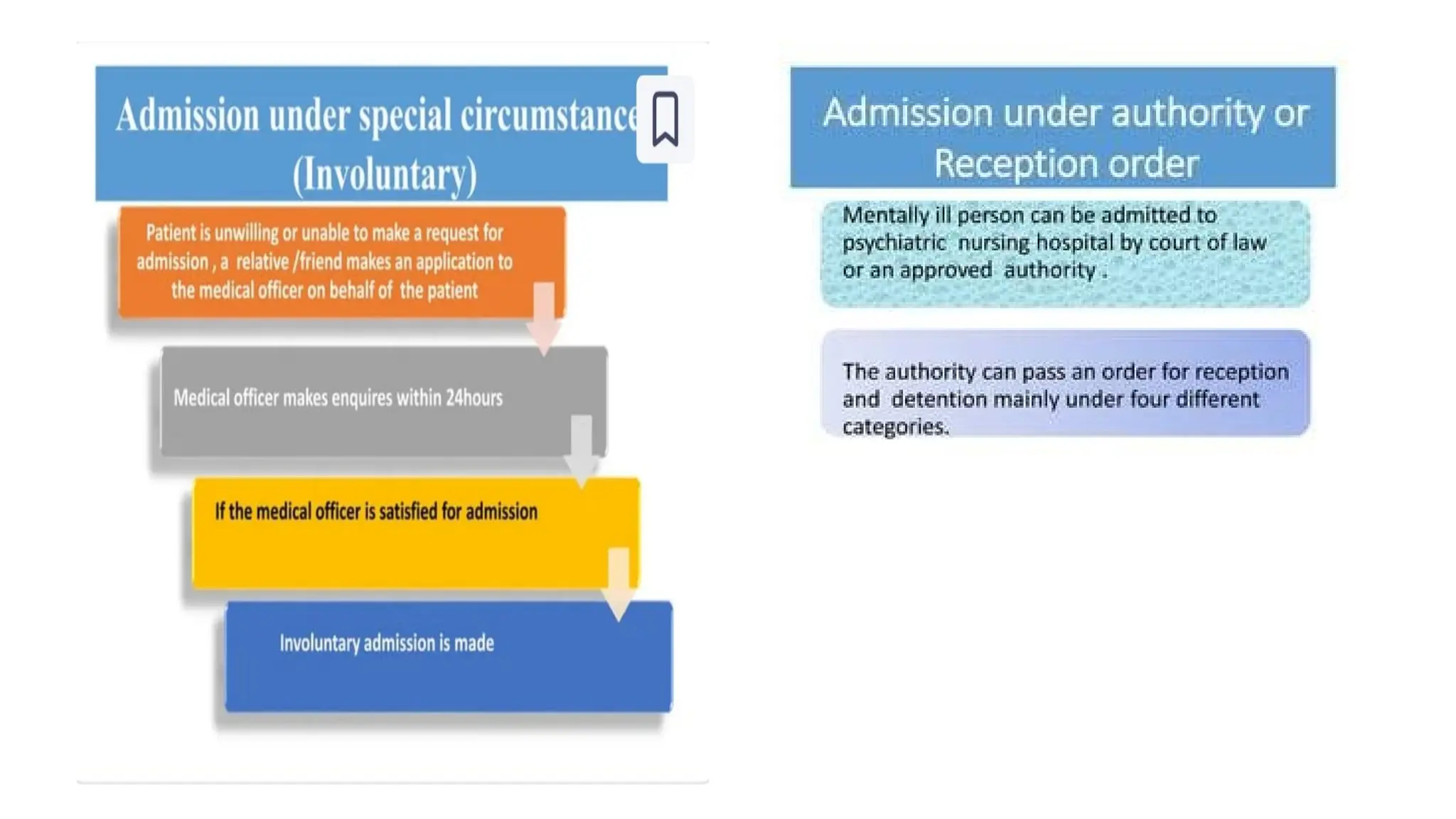
ADMISSION UNDER RECEPTION
ORDER
Onlya relative not other
than husband, wife,
guardian or a friend can
make out an application
for the admission of a
mentally ill patient
application should be
made out to the
magistrate in writing
supported by two
medical certificates,
The patient may now be
admitted after the
magistrate obtains
consent from the
medical officer in-
charge of the mental
hospital
44.
CHAPTER 5
• Thischapter deals with Discharge procedure to be followed in a
mental hospital under different circumstances.
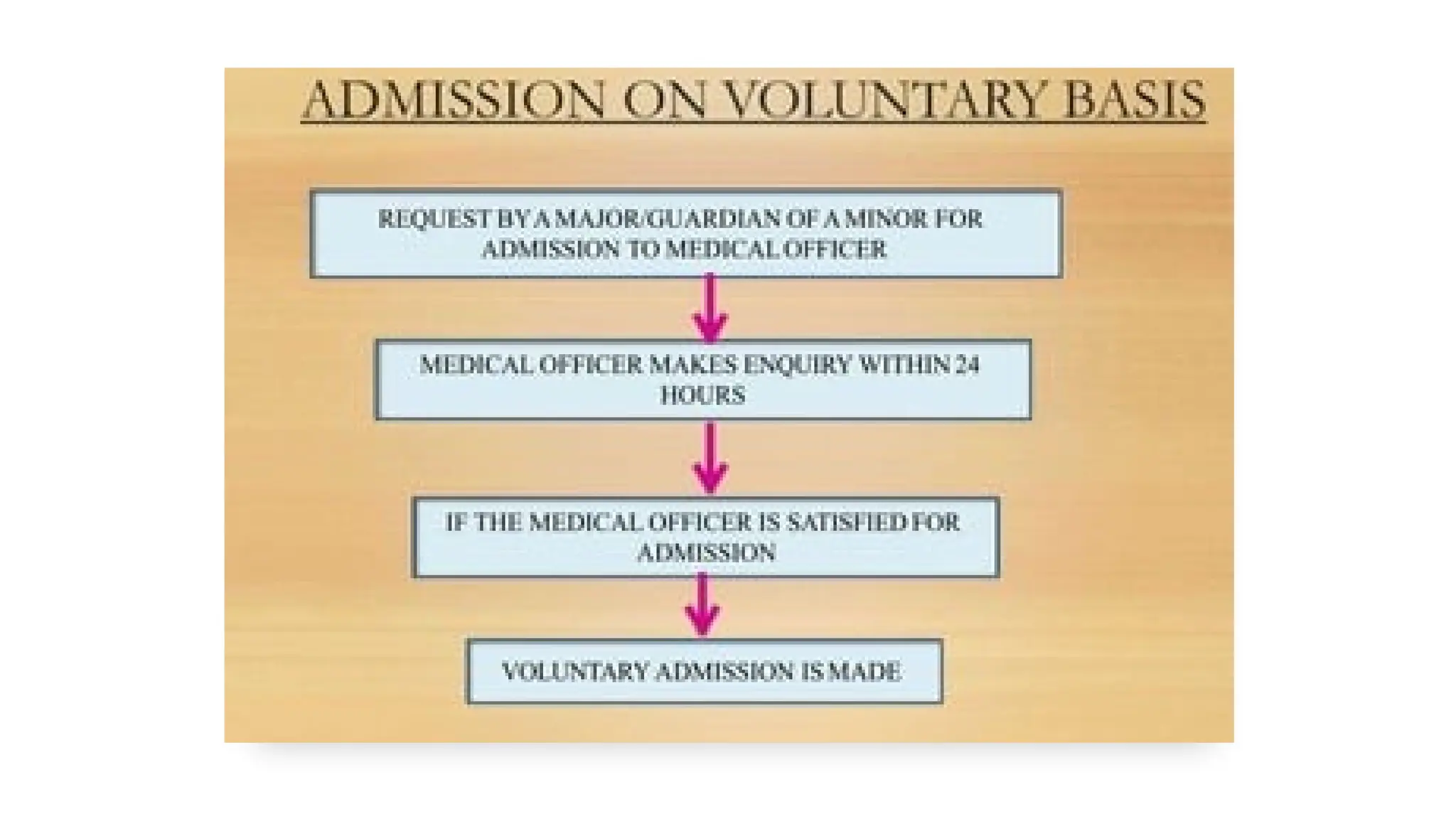
1. ON VOLUNTARY BASIS
• Medical officer in charge of psychiatric hospital on recommendations
with 2 medical practitioner preferably a psychiatrist can issue
directions for the discharge of the patient.
45.
Contd..
2. Discharge OfPatient Admitted Under Special Circumstances
Relative or a friend may make an application to the medical officer
for care and custody of the patient.
Relative are required to furnish our bond with or without along with
an undertaking that the mentally ill person shall be prevented from
causing injury to self or to others.
46.
• CHAPTER 6
Itconsists of legal customary actions towards the property possessed
by mentally ill persons.
• CHAPTER 7
Deals with ways and means to meet the maintenance of mentally ill
person detained in psychiatric hospital.
• CHAPTER 8
Contains some novel and explicit provision for the protection of
human rights of mentally ill person under section 81.
47.
• CHAPTER 9
Dealswith procedure to be followed for the establishment and
maintenance of psychiatric hospitals and penalties which can be
relatively severe and explicit for containing them.
• CHAPTER 10
Deals with clarification pertaining to procedures to be followed by the
medical officer in charge of the psychiatric hospital and psychiatric
homes.
48.
MENTAL HEALTH ACT2017
• The Mental Healthcare Act of
2017 is a significant piece of
legislation passed by the
Government of India aimed at
protecting the rights of
individuals with mental illness
and ensuring they receive
proper care.
• It replaced the Mental Health
Act of 1987
49.
KEY FEATURES
Rights ofPersons with Mental Illness
Decriminalization of Suicide
Advance Directive
Informed Consent and Treatment
Regulation of Mental Health Establishments
Right to Free Legal Aid
Insurance Coverage
50.
RIGHTS UNDER MHA2017
1. Right to Access Healthcare
2. Right to Community Living
3. Right to Protection from Cruelty and Inhumane Treatment
4. Right to Privacy
5. Right to Information
51.
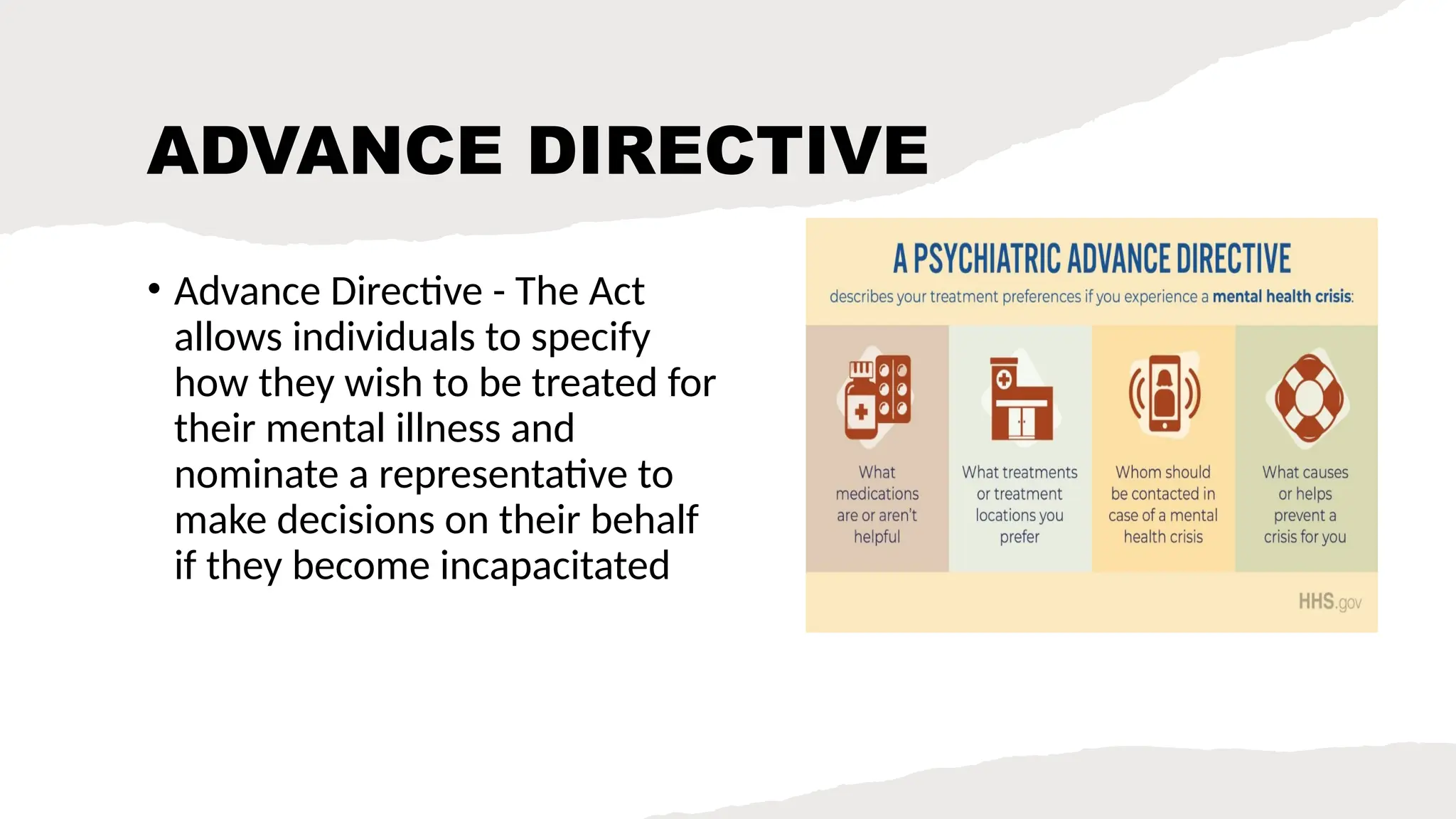
ADVANCE DIRECTIVE
• AdvanceDirective - The Act
allows individuals to specify
how they wish to be treated for
their mental illness and
nominate a representative to
make decisions on their behalf
if they become incapacitated
52.
MHRBs
• Mental HealthReview
Boards are established to
protect the rights of
persons with mental illness,
ensure compliance with the
Act, and hear complaints.
They have the power to
review decisions regarding
the admission, treatment,
and discharge of patients.
53.
DECRIMINALIZATION
OF SUICIDE
• -The Act decriminalizes suicide,
recognizing that a person
attempting suicide should be
presumed to be under severe
stress and should not be
punished but provided with
appropriate care and treatment
• Earlier suicide was considered a
punishable offence under
section 309 of the Indian penal
code
54.
OTHER ADDITIONS..
The useof electroconvulsive therapy (ECT) without anaesthesia is
prohibited, and ECT is banned for minors
Patients are entitled to free legal services and support to ensure
their rights are upheld,
Practices such as chaining and solitary confinement of individuals
with mental illness are strictly prohibited under the Act.
The Act mandates that insurance providers include mental illness in
health insurance policies, providing equal treatment for physical and
mental health conditions.
55.
SIGNIFICANCE
• The MentalHealthcare Act, 2017, represents a paradigm shift in
mental health legislation in India. It moves from a custodial and
punitive approach to a rights-based and person-cantered framework,
aiming to reduce stigma, promote dignity, and ensure comprehensive
care for individuals with mental illness.
56.
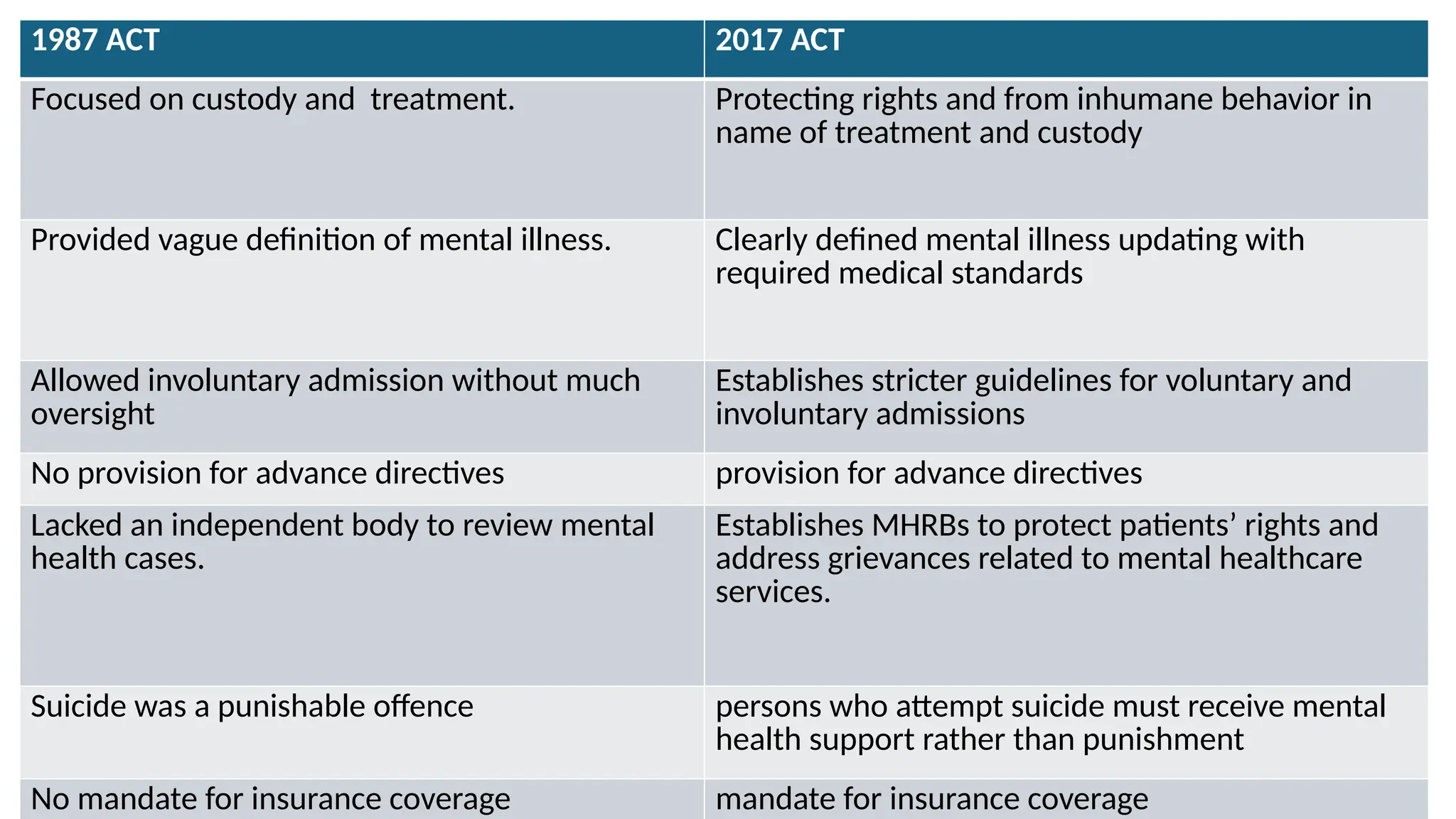
1987 ACT 2017ACT
Focused on custody and treatment. Protecting rights and from inhumane behavior in
name of treatment and custody
Provided vague definition of mental illness. Clearly defined mental illness updating with
required medical standards
Allowed involuntary admission without much
oversight
Establishes stricter guidelines for voluntary and
involuntary admissions
No provision for advance directives provision for advance directives
Lacked an independent body to review mental
health cases.
Establishes MHRBs to protect patients’ rights and
address grievances related to mental healthcare
services.
Suicide was a punishable offence persons who attempt suicide must receive mental
health support rather than punishment
No mandate for insurance coverage mandate for insurance coverage
57.
NARCOTIC DRUGS AND
PSYCHOTROPICSUBSTANCE
ACT 1985
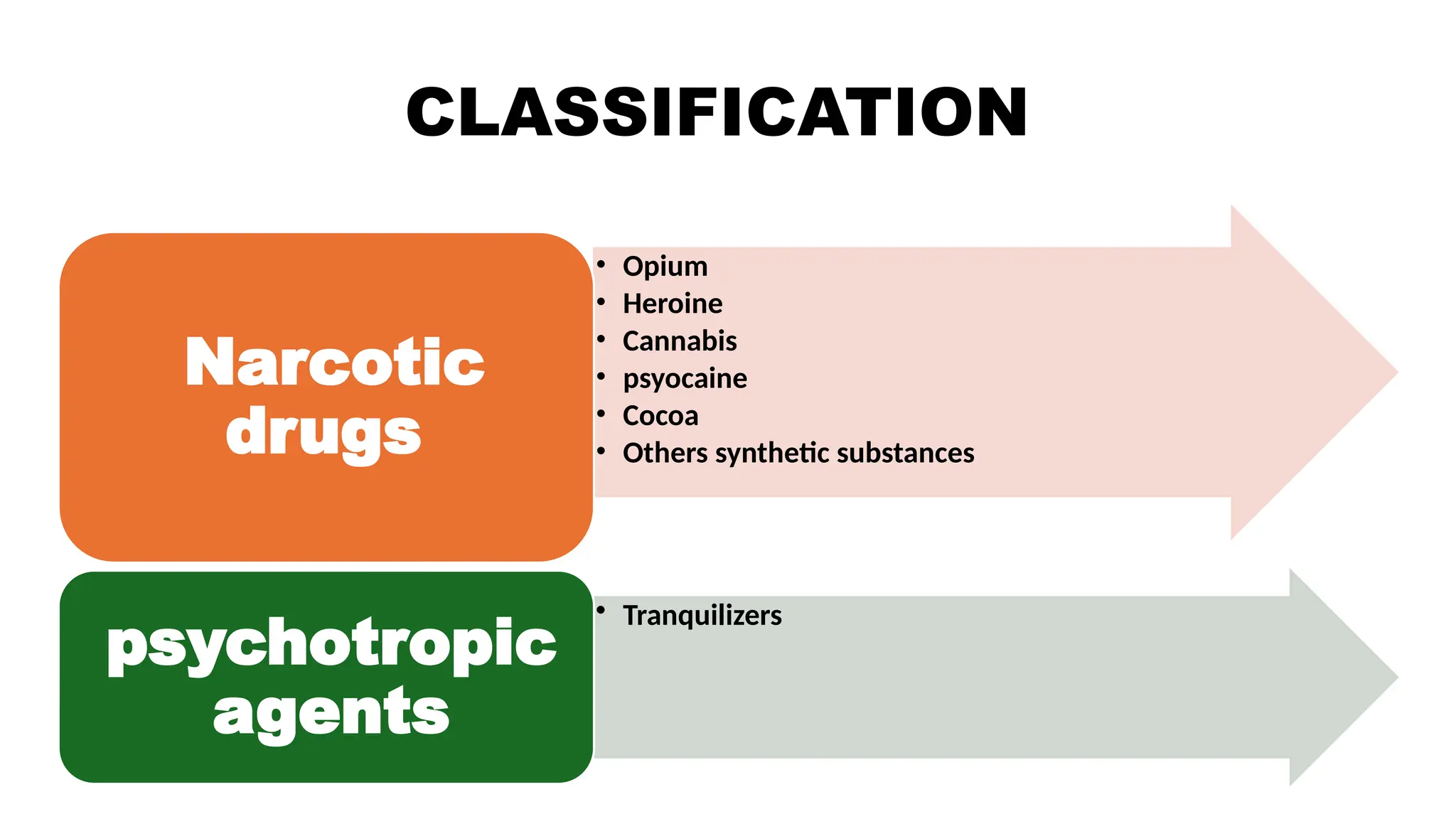
• This act classifies into narcotic
drugs and psychotropic
substances
• This act prohibits the
production, manufacturing,
cultivation, possession, sale,
purchase, transport, storage or
consumption of any narcotic
drugs or psychotropic
substances.
PUNISHMENT
imprisonment of notless than 10 years along with fine not less than
1lakh rupees.
In case of repeated offense rigorous punishment of not less than 15
years along with fine not less than 1.5lakh rupees.
60.
HINDU MARRIAGE ACT1955
Conditions with respect to mental disorders, which must be fulfilled before
the marriage is solemnized under the act, are as follows
1. Neither party is incapable of giving a valid consent as a consequence of
unsoundness of mind
2. Even if capable of giving consent, must not suffer from mental disorders of
such a kind or to such an extent as to be unfit for marriage and the
procreation of children.
3. Must not suffer from recurrent attacks of insanity.
61.
RIGHTS OF
MENTALLY ILL
1.Write to access mental
health care.
2. Right to community living.
3. Right to protection from
inhuman and degrading
treatment.
4. Write to equality and non
discrimination.
5. Right to information
6. Right to confidentiality.
62.
ROLE OF NURSEIN LEGAL
PSYCHIATRY
• Assessment and Documentation
• Patient Advocacy
• Crisis intervention
• Collaboration with Legal Teams
• Rehabilitation and Treatment
Planning
• Education and Training
• Forensic Evaluation Assistance
63.
DO’S OF PSYCHIATRYNURSE
Build Trust and Rapport
Maintain Professional Boundaries
Practice Active Listening
Ensure Patient Safety
Use Therapeutic Communication
Accurate documenting
Respecting patient confidentiality
64.
DONT’S OF PSYCHIATRICNURSE
Judging and stigmatizing
Taking things personally
Using non therapeutic communication
Breaking confidentiality
Ignoring warning signs
Forcing treatment
Making assumptions
Neglecting self care
Being inconsistent
Contd..
Autonomy- Right tomake one’s own decision.
Beneficence- Principle of doing good and what is beneficial to the
patient.
Non maleficence -not to harm the patient. .
67.
Contd..
Veracity-behaviour of honestyand truthfulness in speech.
Fidelity- faithfulness to duties obligations and promises.
Justice equality of benefits to all clients irrespective of their religion,
gender, socio economic status etc.
68.
RESEARCH
INPUT • RESULTS- Overall, 59.5%
of the respondents had
adequate and 40.5% had
inadequate knowledge of
ethical and legal
aspects. There was no
significant association
between the knowledge
score and the selected
variables
69.
NURSING ETHICS IN
COMMUNITYHEALTH
• Nurses practice at a greater level of autonomy.
• Nurses assume greater level of responsibility and accountability.
• Nurses must understand how legislation and policies establish
boundaries for ethical decision making.
• identify and work through ethical dilemmas.
70.
Contd..
• The boundariesmust be maintained in therapeutic relationship with
clients.
• Nurses must take responsibilities for evaluation and maintaining the
boundaries in a nurse client relationship.
• Nurse must value that client with psychiatric disorders are highly
vulnerable.
71.
FORENSIC PSYCHIATRY
• Specialisedbranch of psychiatry
that deals with study diagnosis
and treatment of mental illness
with respect to legal issues.
72.
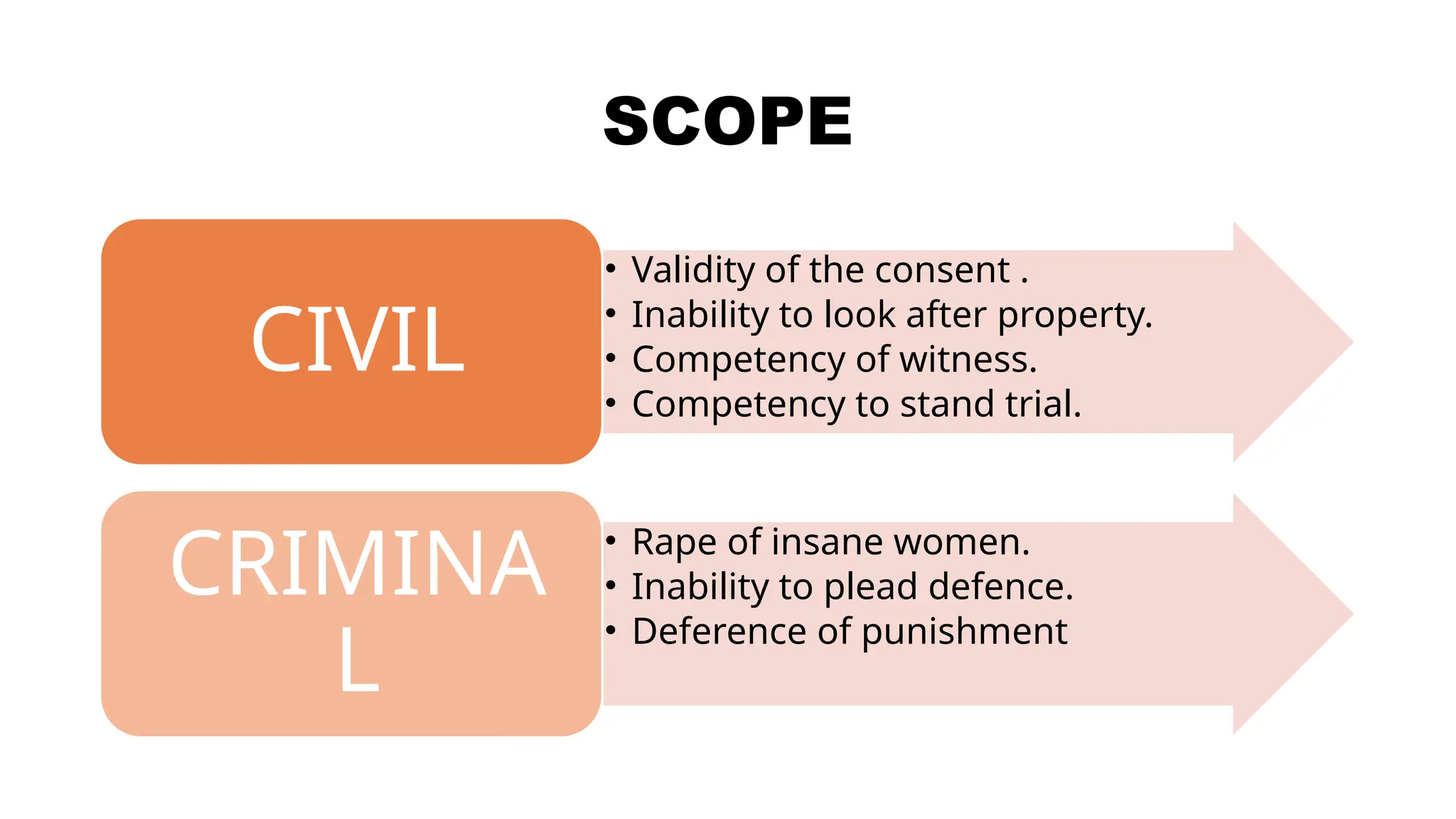
SCOPE
• Validity ofthe consent .
• Inability to look after property.
• Competency of witness.
• Competency to stand trial.
CIVIL
• Rape of insane women.
• Inability to plead defence.
• Deference of punishment
CRIMINA
L
73.
SIGNIFICANCE
Treatment of mentallyill persons who became the perpetrator..
Giving evidence in courts in case when the offender mental stability
is in question.
Competency evaluations.
74.
Contd..
Working effectively tounderstand and upgrade the connection of the
law and psychiatry.
Working with additional clinical and non clinical experts in the field.
Preventing delays in the treatment of offenders with mental
disorders.
75.
RESEARCH INPUT
Results showsthat the majority
(80.0%) of the subjects had
unsatisfactory knowledge regarding
the legal aspects. There is a highly
positive statistically significant
relationship between legal
knowledge and ethical practices
among participating psychiatric
nurses
76.
CONCLUSION
The nurse mustidentify and know all the legal issues specific to her
area of work in order to secure herself and also remain as a client
advocate
She should also inform the client and his relatives about their rights
and keep a check to avoid violation of them by the healthcare team.
Laws pertaining to psychiatry are evolving continuously and demand
protection of client from receiving harm
77.
REFERENCES
1. Wallace M.The legal framework for mental health nursing. Collegian.
1996 Oct;3(4):11-20. doi: 10.1016/s1322-7696(08)60188-2. PMID:
9265522
2. Mitrossili M. [Involuntary treatment of mental patients in the
community: legal and ethical dilemmas]. Psychiatriki. 2014 Oct-
Dec;25(4):285-92. Greek, Modern. PMID: 25630547.
3. Mary. C. Townsend; “psychiatric mental health nursing; 6th
edition”;
page no = 72-82; FA Davis company
78.
Contd..
4. R. Sreevani.A Guide to Mental Health and Psychiatric Nursing.
Delhi: Jaypee brothers; 2017. 215–227 p.
5. Maharjan, S., Thapa, M., & Maharjan, B. (2019). Awareness of
Nurses on Legal and Ethical Aspects of Nursing in Selected Hospitals
of Lalitpur. International Journal of Health Systems and
Implementation Research, 3(2), 25-32. Retrieved from
https://ijhsir.ahsas.

![CIVIL LAW
• Deals with disputes between individuals,
organizations, private rights.
• Primarily focused on providing relief and
compensation to victims.
EXAMPLES
1. Contract disputes
2. Property disputes
3. Family disputes [Divorce]](https://image.slidesharecdn.com/legalasppectts-241211035749-2e90fe0a/75/legal-aspects-of-psychiatric-nursing-pptx-7-2048.jpg)




![REFERENCES
1. Wallace M. The legal framework for mental health nursing. Collegian.
1996 Oct;3(4):11-20. doi: 10.1016/s1322-7696(08)60188-2. PMID:
9265522
2. Mitrossili M. [Involuntary treatment of mental patients in the
community: legal and ethical dilemmas]. Psychiatriki. 2014 Oct-
Dec;25(4):285-92. Greek, Modern. PMID: 25630547.
3. Mary. C. Townsend; “psychiatric mental health nursing; 6th
edition”;
page no = 72-82; FA Davis company](https://image.slidesharecdn.com/legalasppectts-241211035749-2e90fe0a/75/legal-aspects-of-psychiatric-nursing-pptx-77-2048.jpg)